
Figures & data
Figure 1. (A) Hysteroscopy of the cesarean scar defect (CSD). (B) Hysteroscopy after electrical resection of the scar (canal opening) and electrocoagulation of the diverticular endometrium. (C) Laparoscopy of the CSD. (D) Laparoscopic visualization of the diverticulum with guidance from the light source of the hysteroscope after opening and deflecting the vesicouterine pouch. (E) The muscle flap filling suture method: a monopolar electrical probe was used to make a transverse incision in the myometrium 1 cm above the diverticulum to a depth of approximately 0.5 cm. (F) The muscle flap filling suture method. (G) After muscle flap filling suture. (H) The folding suture method. (I) After folding suture.
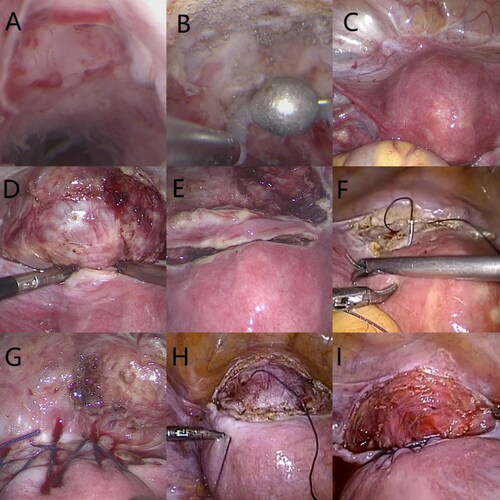
Table 1. Analysis of the basic clinical data of the patients in the two groups
Table 2. Analysis of perioperative clinical data of the patients in the two groups (x ± s).
Table 3. Comparison of surgical efficacy between the patients in the two groups (x ± s).