
Figures & data
Table 1. Patient characteristics and clinical features.
Figure 1. Perifascial areolar tissue was clearly seen over the rectus abdominis fascia.

Figure 2. Preoperative image of the patient who had scald burn. Extensor tendons were exposed and distally with surrounding granulation tissue.

Figure 3. PAT graft application. A: After debridement PAT grafts were adapted to the defect. B: Exposed extensor tendons and distal phalanx components were completely covered with PAT grafts. C: Immediate full-thickness skin grafting after adaptation of PAT grafts.

Figure 4. Post-operative 6th-month image of the patient.

Figure 5. Full-thickness burns of the patient in his hand dorsum after exposure to the radiant heater. The patient had multiple amputations in different levels in his four extremities due to severe peripheral artery disease.

Figure 6. PAT graft application. A: Exposure of second extensor tendons right after debridement. B: PAT grafts were utilized over the exposed tendons.(Dorsum of index digit). C: Split thickness skin grafting was performed simultaneously.
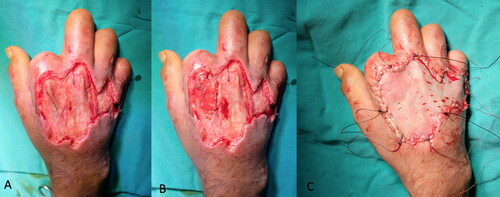
Figure 7. Post-operative 8th-month image of the patient.

Figure 8. The patient sustained from high-voltage electric burns in his lower extremity and right hand. Although he had a muscle flap reconstruction and skin grafting previously, there was still anterior tibial muscle tendon and tibial bone exposure at the injured site.

Figure 9. PAT graft application. A: 6 × 4 cm sized PAT graft was harvested from the abdominal region. B: PAT grafts were adapted to cover the exposed anterior tibial bone and tendon. C: 3:1 meshed split-thickness skin grafting was performed over PAT grafts and the rest of the defect.

Figure 10. Post-operative first-year image of the patient demonstrates no existing functional deficit in foot dorsiflexion (C) and plantar flexion (B) movements.

Figure 11. Different from the literature, we advocate more superior incision for PAT graft harvesting in order to protect superficial circumplex epigastric artery based flaps which may be needed in later stages of burn reconstruction.
