
Figures & data
Table 1. The clinical characteristics of patients in the two groups.
Table 2. The general results in two groups during their duration of hospital stay.
Table 3. The radiological results and clinical outcomes in two groups at admission, after operation and at the last follow up.
Figure 1. Case 1. A 74-years old female patient complained refractory low back pain after lumbar sprain 90 days ago. A-B: X-ray at admission demonstrated L2 compression fracture with narrowed L1/2 disk space. C: Preoperative CT sagittal reconstruction show L2 collapse and osteophyte formation with upper endplate fracture. D: MRI at admission showed severe compressed and subacute fracture of L2, L1/2 disk space at T2 WI show disk injury with heterogeneous signal. E: Unilateral extra-pedicular PKP was performed at the injured vertebra, fluoroscopy show cement leak into the injured disk after adequate distribution in the L2. F-G, H: Postoperative X-ray and CT sagittal reconstruction show adequate cement distribution in the injured vertebra and disk, the cement bridge is generated between the vertebra and disk..

Figure 2. Case 1. A 74-years old female patient complained refractory low back pain after lumbar sprain 90 days ago. A: Preoperative full-length spine X-ray of the same patient show local kyphosis angle is 24.1°, the sagittal vertical axis(SVA) is -29.9 mm B: at the last follow up(35 months after operation), full-length spine X-ray show local kyphosis angle is 11.9°, the sagittal vertical axis(SVA) is 19.8 mm, the cement keeps in the original place.
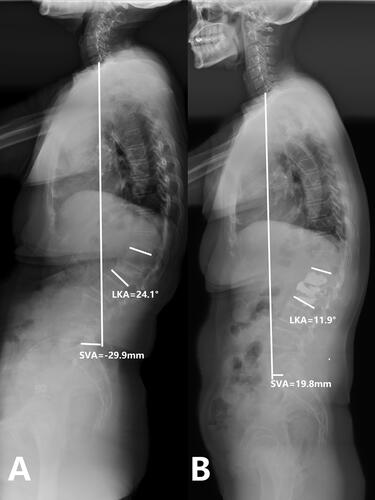
Figure 3. Case 2. PSV + VP. A 69-years old female patient complained refractory low back pain with functional dyspepsia which was persistent for about 6 months without any injury. A-B: X-ray at admission demonstrated L1 compression fracture with narrowed L1/2 disk space. C: Preoperative CT sagittal reconstruction show L1 collapse and intra-vertebral vacuum cleft with upper endplate fracture. D: MRI at admission showed severe compressed intra-vertebral vacuum cleft of L2, L1/2 disk space at T2 WI show disk injury with heterogeneous signal. E-F,G: Postoperative X-ray and CT sagittal reconstruction show adequate cement distribution in the injured vertebra, with bone cement reinforced screws fixation at the adjacent vertebrae.

Figure 4. Case 2. PSV + VP. A 69-years old female patient complained refractory low back pain with functional dyspepsia which was persistent for about 6 months without any injury. A: Preoperative full-length spine X-ray of the same patient show local kyphosis angle is 25.2°, the sagittal vertical axis(SVA) is -47.8 mm. B: at the last follow up(33 months after operation), full-length spine X-ray show local kyphosis angle is 15.2°, the sagittal vertical axis(SVA) is 11.7 mm, the cement and internal fixation keeps in the original place.
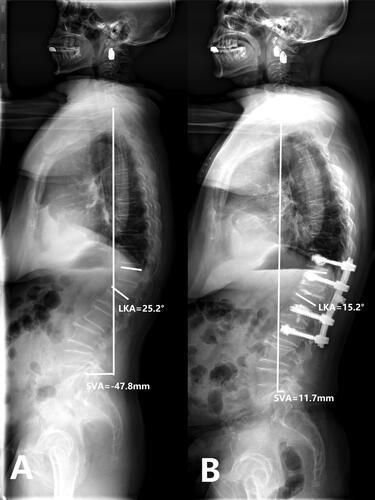
Table 4. The complications in two groups at Peri-operative period and at the last follow up.