Figures & data
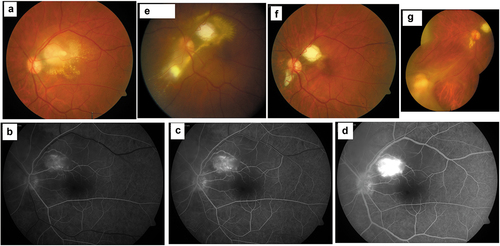
Figure 1. Case of a migrating Toxocara granuloma.
A 31-year-old man presented with a 3-month history of diminution of vision from his left eye. Visual acuity was CF+ with LE RAPD and inflammatory cells in the anterior chamber and the vitreous cavity. He was diagnosed as neuroretintis. (Figure 1a) Fundus fluorescein angiography revealed angiomatous proliferation within the lesion. (Figures1b-d) Lab investigations were non-contributory. He was treated with oral clindamycin and Bactrim-DS without any response. He underwent pars plana vitreous surgery twice over during the next several months. Six months from presentation a fresh retinitis lesion was noted lower nasal to the optic disc with a subretinal track leading from the original lesion that had scarred by now. (Figure 1e) Nearly two years later the lesions had stabilized (Figure 1 f). Four years later, a fresh granuloma was noted in the lower nasal periphery with a subretinal track from the previous scar and a tractional retinal detachment (Figure 1 g).