Figures & data
Table 1. Ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome.
Table 2. Ultrasound findings by age group.
Table 3.. Detailed ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome..
Table 4. Bilateral ultrasound findings of structural abnormalities in 115 patients with unilateral subacromial pain syndrome, presented in age intervals.
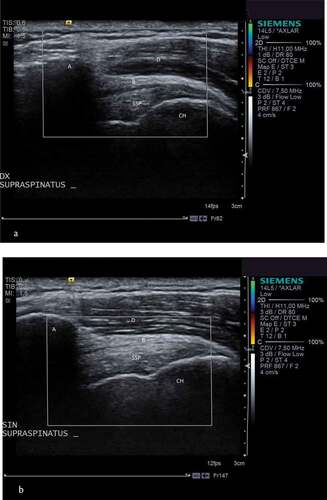
Figure 1. A and b. Ultrasound of both shoulders in a 43 year old female patient with unilateral subacromial pain syndrome.
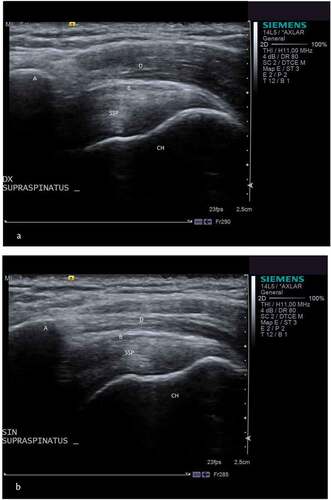
Figure 2. A and b. Ultrasound of both shoulders in a 48 year old female patient with unilateral subacromial pain syndrome.

Figure 3. A and b. Ultrasound of both shoulders in a 33 year old male patient with unilateral subacromial pain syndrome.

Figure 4. A and b. Ultrasound of both shoulders in a 42 year old male patient with unilateral subacromial pain syndrome.
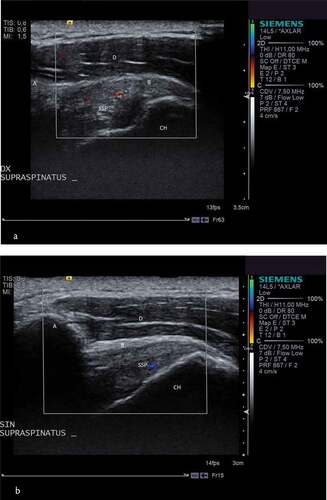
Figure 5. A and b. Ultrasound of both shoulders in a 53 year old male patient with unilateral subacromial pain syndrome.