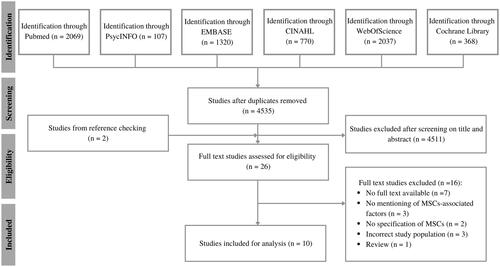
Figure 1. Flowchart for the selection of studies according to the PRISMA guidelines. MSCs: musculoskeletal complaints.
The first phase in selecting studies is identification. Six databases were searched, resulting in respectively 2069, 107, 1320, 770, 2037, and 368 articles. The number of studies after duplicates were removed (n = 4535) went onto the second stage, which was screening on title and abstract. After removing 4511 studies and adding two studies from reference checking, 26 articles were assessed for eligibility with full text screening (third phase). Sixteen studies were excluded, resulting in 10 studies being included for analysis (fourth and final phase).
Long description. The first phase in selecting studies is identification. Six databases (PubMed, PsycINFO, EMBASE, CINAHL, Web of Science, and Cochrane Library) were searched, resulting in respectively 2069, 107, 1320, 770, 2037, and 368 articles. The number of studies after duplicates were removed (n = 4535) went onto the second stage, which was screening on title and abstract. After removing 4511 and adding two studies from reference checking, 26 articles were assessed for eligibility with full text screening (third phase). Sixteen studies were excluded, exclusion reasons were: no full text available (n = 7), no mentioning of MSCs-associated factors (n = 3), no specification of MSCs (n = 2), incorrect study population (n = 3), and a review (n = 1). Ultimately, 10 studies were included for analysis (fourth and final phase).
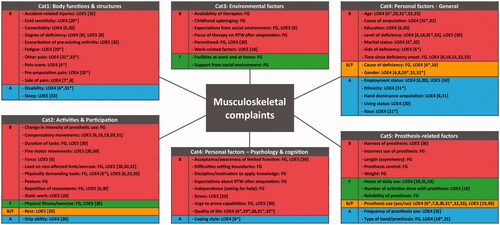
Figure 2. Final overview of factors associated with musculoskeletal complaints in persons with upper limb absence. Divided into barriers (B, red), facilitators (F, green), both barriers and facilitators (B/F, orange), and association undefined (A, blue). Factors were categorized as a barrier if the focus group or the studies mentioned, hypothesized, or analyzed that the factor increases MSCs. Factors that reduced MSCs were categorized as facilitators. If there were contradicting results between the focus group or studies, the factor was classified as both. The remaining associated factors consist of factors of which the association was undefined in the focus group and all studies. References with significant results are displayed with a *. Cat: category; B: barrier; F: facilitator; B/F: barrier and facilitator; A: association undefined; FG: focus group qualified as evidence level 5; LOE4: scoping review results qualified as evidence level 4; LOE5: scoping review results qualified as evidence level 5; RTW: return to work.
Overview of 66 factors for MSCs divided over five main categories: (1) body functions and structures; (2) activities and participation; (3) environmental factors; (4) personal factors (subcategories: psychology and cognition, and general); and (5) prosthesis-related factors. Each category has a list of factors divided into barriers, facilitators, both, or association undefined. Each factor describes the level of evidence (FG, LOE4, or LOE 5) with the references.
Long description. Overview of 66 factors for MSCs divided over five main categories and categorized as barriers, facilitators, both, or association undefined. Each factor describes the level of evidence (FG, LOE4, or LOE 5) with the references. Category 1 “Body functions and structures” consists of 10 barriers (accident-related injuries, cold sensitivity, comorbidity, degree of deficiency, exacerbation of pre-existing arthritis, fatigue, other pain, pain score, pre-amputation pain, and side of pain) and two associations (disability and sleep). Category 2 “Activities and participation” consists of 10 barriers (change in intensity of prosthetic use, compensatory movements, duration of tasks, fine motor movements, force, load on non-affected limb/overuse, physically demanding tasks, posture, repetition of movements, and static work), one facilitator (physical fitness/exercise), one that is both a barrier and facilitator (rest), and one association (grip ability). Category 3 “Environmental factors” has six barriers (availability of therapies, childhood upbringing, expectations from social environment, focus of therapy on RTW after amputation, parenthood, and work-related factors) and two facilitators (facilities at work and at home, and support from social environment). Category 4 “Personal factors”, with subcategory “Psychology and cognition” describes eight barriers (acceptance/awareness of limited function, difficulties setting boundaries, discipline/motivation to apply knowledge, expectations about RTW after amputation, independence (asking for help), stress, urge to prove capabilities, and quality of life) and one association (coping style). The subcategory “General” of the main category 4 “Personal factors” lists seven barriers (age, cause of amputation, education, level of deficiency, marital status, side of deficiency, and time since deficiency onset), two factors that are both barriers and facilitators (cause of deficiency, and gender), and five associations (employment status, ethnicity, hand dominance amputation, living status, and race). Lastly, category 5 “Prosthesis-related factors” consists of five barriers (harness of prosthesis, incorrect use of prosthesis, length (asymmetry), prosthesis control, and weight), three facilitators (hours of daily use, number of activities done with prosthesis, and reliability of prosthesis), one that is both (prosthesis use (yes/no)), and two associations (frequency of prosthesis use, and type of hand/prosthesis).
Postema SG, Bongers RM, Brouwers MA, et al. Musculoskeletal complaints in transverse upper limb reduction deficiency and amputation in The Netherlands: prevalence, predictors, and effect on health. Arch Phys Med Rehabil. 2016;97(7):1137–1145.
Johansen H, Østlie K, Andersen LØ, et al. Adults with congenital limb deficiency in Norway: demographic and clinical features, pain and the use of health care and welfare services. A cross-sectional study. Disabil Rehabil. 2015;37(22):2076–2082.
Johansen H, Østlie K, Andersen LØ, et al. Health-related quality of life in adults with congenital unilateral upper limb deficiency in Norway. A cross-sectional study. Disabil Rehabil. 2016;38(23):2305–2314.
Johansen H, Bathen T, Andersen LØ, et al. Chronic pain and fatigue in adults with congenital unilateral upper limb deficiency in Norway. A cross-sectional study. PLOS One. 2018;13(1):e0190567.
Resnik L, Borgia M, Clark MA. The prevalence and impact of back and neck pain in veterans with upper limb amputation. Am J Phys Med Rehabil. 2021;100(11):1042–1053.
Jones LE, Davidson JH. Save that arm: a study of problems in the remaining arm of unilateral upper limb amputees. Prosthet Orthot Int. 1999;23(1):55–58.
Desmond DM, Maclachlan M. Prevalence and characteristics of phantom limb pain and residual limb pain in the long term after upper limb amputation. Int J Rehabil Res. 2010;33(3):279–282.
Østlie K, Franklin RJ, Skjeldal OH, et al. Musculoskeletal pain and overuse syndromes in adult acquired major upper-limb amputees. Arch Phys Med Rehabil. 2011;92(12):1967–1973.e1.
Burger H, Vidmar G. A survey of overuse problems in patients with acquired or congenital upper limb deficiency. Prosthet Orthot Int. 2016;40(4):497–502.