
Figures & data
Figure 1. Consort diagram of our cross-sectional study. N = 172 participants were screened for eligibility in the study, with 172 meeting initial inclusion/exclusion criteria and approached for consent. N = 141 participants consented to participation (81.9%) with 99 returning for the in-person clinical interview (69.5%). N = 88 (89.8%) participants with usable data necessary for PTSD symptom severity analysis, N = 66 for the RSA analysis, and N = 61 for the DES analysis.
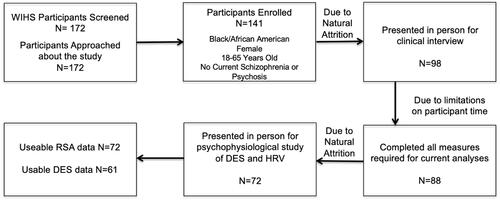
Table 1. Demographic characteristics for overall study sample.
Figure 2. Effects of HIV status and childhood maltreatment on CAPS-5 PTSD symptom severity. HIV was associated with greater PTSD symptoms severity only in women with low levels of childhood maltreatment (p=.030). In women without HIV, high versus low childhood maltreatment was also associated with greater PTSD symptom severity (p<.001).
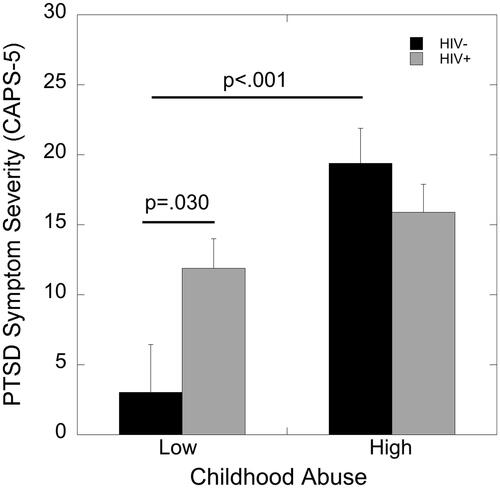
Figure 3. Effects of HIV status and childhood maltreatment on percent potentiation due to darkness during the DES paradigm. Childhood maltreatment was associated with greater percent potentiation to darkness in women living without HIV (p=.018) but not in WLWH (p=.49).
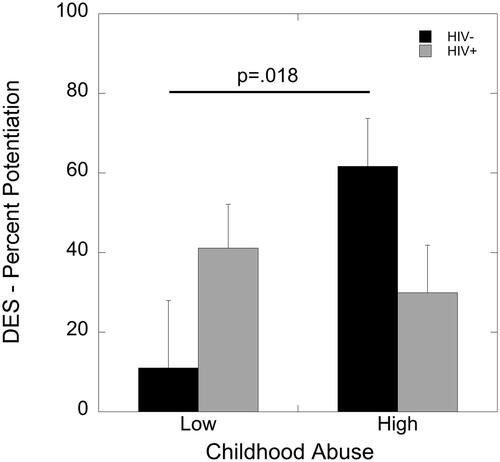
Figure 4. Effects of HIV status, childhood maltreatment, and phase of DES (light vs. dark) on RSA. RSA was significantly lower during the dark compared to the light phase of the DES task in women without HIV who had experienced low levels of childhood maltreatment (p=.046). WLWH with low childhood maltreatment showed significantly lower RSA during the light phase of the DES compared to women without HIV (p=.042).
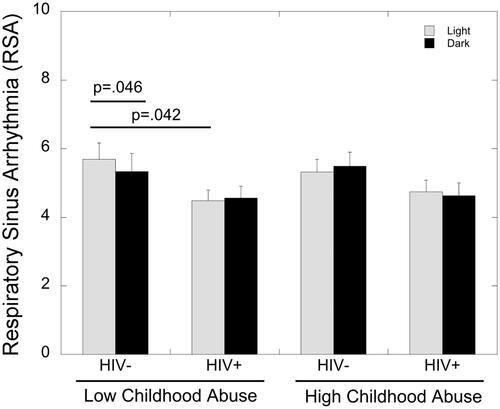
Table 2. Summary of study findings broken down by HIV status (HIV + vs HIV-) and childhood maltreatment (Low vs. High). Significant differences are denoted by comparisons and lack of differences by dashes.