
Figures & data
Figure 1. Microscopic pictures of myeloid neoplasms with STAT5B mutations (A–F) and bone marrow of a patient with peripheral T-cell lymphoma (PTCL)-NOS with STAT5B mutation (G–H). (A) Marrow shows sheets of myeloblasts (Case #1, Bone marrow biopsy, HE ×400), (B) pSTAT5 immunohistochemistry shows immunoreactivity in myeloblasts (Case #1, Bone marrow biopsy, pSTAT5 × 400), (C) eosinophils and precursors are increased (Case #4, Bone marrow biopsy, HE x400), (D) peripheral blood shows increase in eosinophils (Case #4, Peripheral blood, Giemsa x500), (E) eosinophils and precursors are increased (Case #5, Bone marrow biopsy, HE ×400), (F) CD61 highlights numerous dysplastic megakaryocytes (Case #5, Bone marrow biopsy, CD61 × 200), (G) bone marrow shows increased eosinophils and precursors (PTCL-NOS, Bone marrow biopsy, HE ×200), (H) peripheral blood shows increase in eosinophils (PTCL-NOS, Peripheral blood, Giemsa ×500), (I) flow cytometry performed with bone marrow aspirate sample of PTCL-NOS patient shows small abnormal T-cell population with loss of surface CD3 (0.26% of total WBC), consistent with minimal bone marrow involvement by PTCL-NOS. (J) flow sorting was performed with a peripheral blood sample of Case #4 to isolate granulocytes, eosinophils, B-cells and T-cells to further perform NGS in each population, (K) The results of subsequent next generation sequencing in each population of Case #4. STAT5B mutations were identified in granulocytes and eosinophils, but not in B-cells or T-cells.
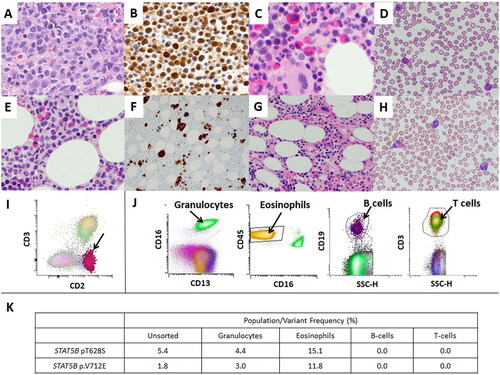
Table 1. Myeloid neoplasms with STAT5B mutations.