
Figures & data
Figure 1. Anatomy of knee joint (KNJ) and temporomandibular joint (TMJ) in pigs. A–C: Anatomy of KNJ. a. Medial femoral condyle; b. Lateral femoral condyle; c. Femoral pulley; d. Lateral collateral ligament; e. Medial collateral ligament; f. Anterior cruciate ligament; g. Posterior cruciate ligament; h. Medial meniscus; i. Lateral meniscus; j. Subpatellar fat; k. Patella. D–F. Anatomy of TMJ. l. Mandibular condyle; m. Articular disk; n. Articular fossa; o. Coracoid process; p. Mandibular body; G. Embryo on E35; H. Embryo on E90; I. Embryo on P0
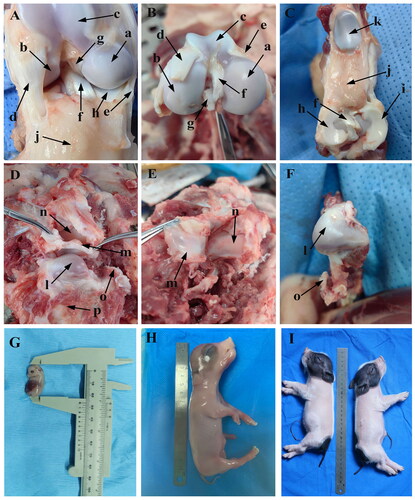
Figure 2. Sagittal histological section of Knee joint (KNJ) with hematoxylin–eosin and Safranin O-fast green staining on E30. The interzone and popliteal muscle mesenchymal condensate begin to appear in KNJ. Tibialis anterior muscle has been formed. The femur, tibial shaft and acetabulum begin to become cartilaginous. Chondrocytes are arranged in layers, and the cavitation cells can be seen in the tibia, femur and acetabulum. There is a long fissure between the head of the femur and the acetabulum. 1) magnify to E; 2) magnify to F. a,b. Mesenchymal condensate; c. Femoral shaft; d. Tibia shaft; e. Femoral head; f. Acetabulum; g. Articular cavity; h. Vertebra; i. Tarsal bone; j. Tibialis anterior muscle; k. Popliteal muscle mesenchymal condensate; l. Chondrocytes; m. Cavitating chondrocytes.
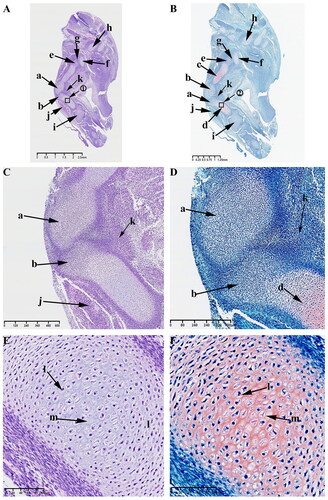
Figure 3. Sagittal histological section of Knee joint (KNJ) and Temporomandibular joint (TMJ) with hematoxylin–eosin and Safranin O-fast green staining on E35. The knee mesenchymal condensate is separated from the middle. The articular cavity is formed by cavitation between the femur and tibia. Chondrocytes surrounded by stem cells line the femur and tibia in a vortex. Cavitation occurs in some chondrocytes. Two mesenchymal condensates start to appear in the TMJ. Chondrification of the TMJ occurs in the temporal region. The cells line up in a vortex, and the chondrocytes in the center of the vortex begin to cavitate. There is no chondrification in the mandibular condyle. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. 1) magnify to E; 2) magnify to F; 3)magnify to I; 4) magnify to J; 5) magnify to K; 6) magnify to L. a. Femur; b. Tibia; c. Femoral head; d. Acetabulum; e. Tarsal bone; f. Lateral vastus muscle; g. Tibialis anterior muscle; h. Articular cavity; i. Chondrocytes; j. Cavitating chondrocytes; k. Temporal primordium; l. Condylar primordium; m. brain; n. eye; o. mouth; p. Meckel’s cartilage; q. Pharyngeal cavity; r. External auditory canal; s. Chondrocytes; t. Cavitating chondrocytes.
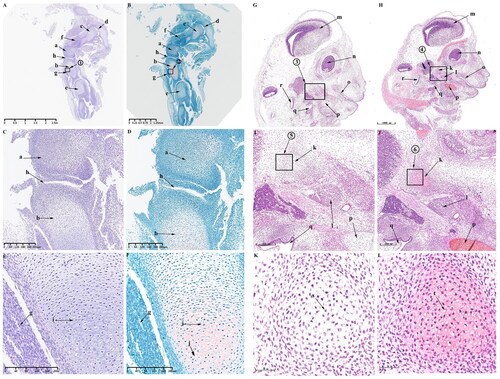
Figure 4. Sagittal histological section of KNJ and TMJ with hematoxylin–eosin and Safranin O-fast green staining on E45. The meniscus and articular eminence are clearly visible. The patella develops and begins to become cartilaginous. There is a concentrated zone of chondrocytes which develop into epiphyseal plates below the chondrocyte layer of the femur and tibia, and the cells are fusiform. The superior and inferior articular cavities of the TMJ have been formed. There is still fibrous tissue in the superior and inferior articular cavities. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. a. Femoral condyle; b. Tibial plateau; c. Patella; d. Patellar ligament; e. suprapatellar bursa; f. Meniscus; g. Eminence of medial joint; h. Soleus muscle; i. Popliteal muscle; j. Tibialis anterior muscle; k. Mineralized area; l. Growth plate; m. Eminence of lateral joint; n. Chondrocytes; o. Growth plate; p. Hypertrophic chondrocytes; q. Condyle; r. Temporal bone; s. Cartilage canal; t. Inferior articular cavity; u. Superior articular cavity; v. Articular disk; w. Round chondrocytes; x. Fusiform chondrocytes y. Hypertrophic chondrocytes.
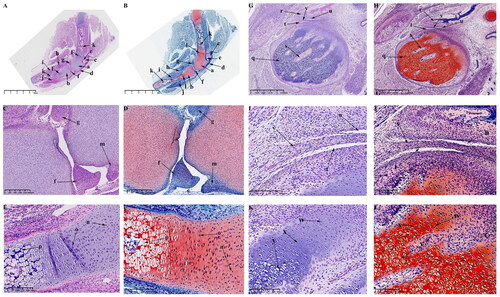
Figure 5. Sagittal histological section of KNJ and TMJ with hematoxylin–eosin and Safranin O-fast green staining on E55. The tibia and femur are still rich in chondrocytes, forming vascular-rich cartilage canals in the group of chondrocytes to provide nutrition for chondrocytes. During the development of TMJ, the temporal bone is completely ossified. The mandibular condyle is typically oval. The articular disk, superior articular cavity and inferior articular cavity have been formed. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. 1) magnify to E; 2) magnify to F; 3) magnify to K; 4) magnify to L. a. Femur; b. Tibia; c. Patella; d. Meniscus; e. Cartilage canal; f. Infrapatellar fat pad; g. Tendon of quadriceps femoris; h. Mineralized area; i. Anterior cruciate ligament; j. Oval chondrocytes; k. Round chondrocytes; l. Hypertrophic chondrocytes; m. Mineralized area; n. Temporal bone; o. Mandibular condyle; p. Articular disk; q. superior articular cavity; r. inferior articular cavity; s. Fusiform chondrocyte; t. Oval chondrocytes; u. Hypertrophic chondrocytes.
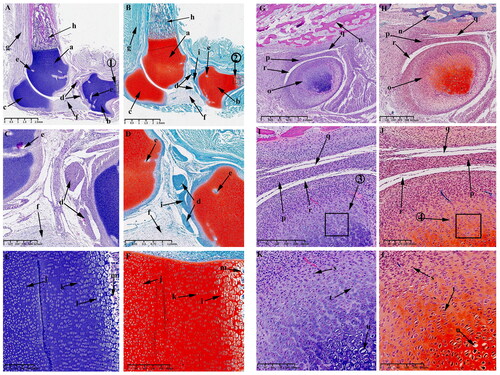
Figure 6. Sagittal histological section of knee joint (KNJ) and temporomandibular joint (TMJ) with hematoxylin–eosin and Safranin O-fast green staining on E75. The meniscus, cruciate ligament, infrapatellar fat pad and intercondylar process are clearly visible. The growth plate is more obvious. There are four chondrocytes types in the growth plate. The chondrocytes above the growth plate are rounded and irregularly arranged. The chondrocytes of the second layer are tightly packed in clusters, and those of the third layer are closely aligned in rows. The lowest-lying chondrocytes have hypertrophy and cavitation. Mineralization occurs below the condylar cartilage layer in the TMJ. The cartilage canal in TMJ extends along the longitudinal axis of the condyle, dividing the condyle into several parts, while the cartilage canal in the KNJ is arranged vertically and horizontally. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. 1) magnify to E; 2) magnify to F; 3) magnify to K; 4) magnify to L. a. Femur; b. Tibia; c. Patella; d. Meniscus; e. Anterior cruciate ligament; f. Patellar ligament; g. Cartilage canal; h. Infrapatellar fat pad; i. Intercondylar eminence; j. Growth plate; k. Popliteal muscle; l. Tibialis anterior muscle; m. Round chondrocytes; n. Clusters of chondrocytes; o. Columnar arranged chondrocytes; p. Hypertrophic chondrocytes; q. Mineralized area; r. Temporal bone; s. Mandibular condyle; t. Articular disk; u. superior articular cavity; v. inferior articular cavity; w. Mineralized area; x. Fibrous tissue; y. Cartilage canal; z. Chondrocytes; z1. Hypertrophy chondrocyte.
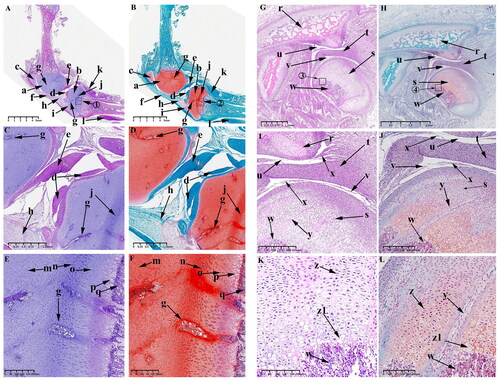
Figure 7. Sagittal histological section of knee joint (KNJ) and temporomandibular joint (TMJ) with hematoxylin–eosin and Safranin O-fast green staining on E90. The 90th day of embryonic development is the further maturation stage of KNJ and TMJ. The development of KNJ and TMJ is similar to that of E55. The most pronounced feature on E90 is the production of more cartilage canals in each chondrocyte region. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. 1)magnify to E; 2)magnify to F; 3)magnify to K; 4)magnify to L. a. Femur; b. Tibia; c. Patella; d. Meniscus; e. Cruciate ligament; f. Infrapatellar fat pad; g. Cartilage canal; h. Chondrocytes; i. Chondrocyte hypertrophy; j. Mineralized area; k. Temporal bone; l. Mandibular condyle; m. Articular disk; n. superior articular cavity; o. inferior articular cavity; p. Chondrocytes; q. Hypertrophy chondrocyte; r. Cartilage canal.
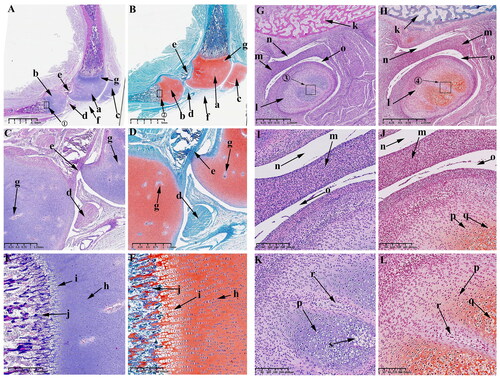
Figure 8. Sagittal histological section of Knee joint (KNJ) and temporomandibular joint (TMJ) with hematoxylin–eosin and Safranin O-fast green staining on P0. The secondary ossification center of KNJ are established in the epiphysis of the femur and tibia. There was no secondary ossification center in the mandibular condyle. A–F. Histological analysis of KNJ; G–L. Histological analysis of TMJ. 1) magnify to C; 2) magnify to E; 3) magnify to D; 4) magnify to F; 5) magnify to K; 6) magnify to L. a. Femoral epiphysis; b. Tibia epiphysis; c. Meniscus; d. Cruciate ligament; e, f. Growth plate; g. Patellar ligament; h. Articular surface cartilage; i. Patella; j. Infrapatellar fat; k. Prechondral cell; l. Chondrocytes; m. Hypertrophic chondrocytes; n. Mineralized area under the growth plate; o. Growth plate chondrocytes; p. Growth plate chondrocyte hypertrophy; q. Hypertrophy chondrocytes on the joint surface; r. Bone marrow cavity; s. Mineralized area above the growth plate; t. chondrocytes on the joint surface u. Mandibular condyle; v. Mineralized area; w. Articular disk; x. Superior articular cavity; y. inferior articular cavity; z. Bone marrow cavity; a1, Chondrocytes; b1, Hypertrophic chondrocytes; c1, Mineralized area.
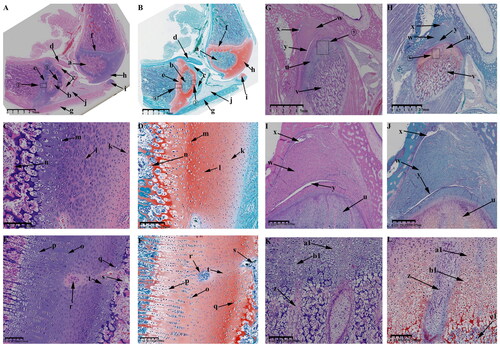
Figure 9. Sagittal histological section of Knee joint (KNJ) and Temporomandibular joint (TMJ) with hematoxylin–eosin and Safranin O-fast green staining on P30. The growth plate is still attached to the femoral condylar cartilage at the edges. Chondrocytes of the growth plate are densely packed and arranged along the longitudinal axis of the femoral and tibia condyles. In the development of TMJ, the chondrocyte layer of the mandibular condyle becomes thinner. The condyle is divided into several parts by multiple cartilage canals. There is no growth plate formation in TMJ. A-F. Histological analysis of epiphysis; G–L. Histological analysis of proximal tibia; M–R. Histological analysis of mandibular condyle. 1) magnify to B; 2) magnify to C; 3) magnify to E; 4) magnify to F; 5) magnify to I; 6) magnify to H; 7) magnify to L; 8) magnify to K; 9) magnify to N; 10) magnify to O; 11) magnify to Q; 12) magnify to R. a. Growth plate; b. Chondrocyte layer of femoral condyle; c. Cartilage canal; d. Ossification area of femoral condyle; e. Ossification area of femoral shaft; f. Growth plate chondrocytes arranged in rows; g. Growth plate chondrocytes; h. Hypertrophic chondrocytes; i. Surface cells of femoral condyle; j. Chondrocytes of femoral condyle; k. Hypertrophic chondrocytes of femoral condyle; l. The growth plate of the tibia; m. Surface cell layer of tibia; n. Meniscus; o. Ossification area of tibial condyle; p. Ossification area of tibial shaft; q. Chondrocytes of tibial growth plate; r. Chondrocytes of tibial condyle; s. Hypertrophic chondrocytes of tibial growth plate; t. Hypertrophic chondrocytes of tibia; u. Mandibular condyle; v. Coracoid process of mandible; w. Cartilage canal; x. prechondrocytes; y. Condylar chondrocytes; z. Hypertrophic chondrocytes.
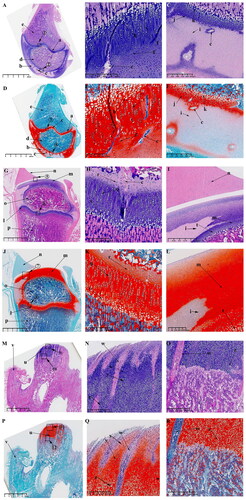
Table 1. The important events during the embryonic development of KNJ and TMJ in this study.