Figures & data
Table 1. Demographic and clinical characteristics, Lesion characteristics and treatment results of the cases.
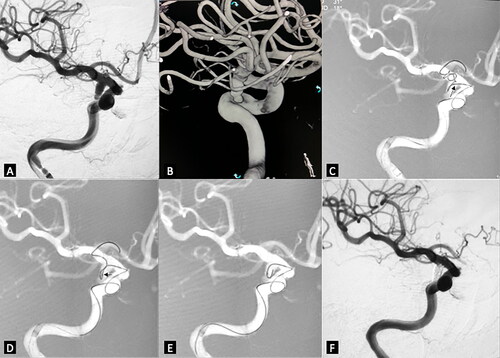
Figure 1. Embolization of irregular posterior cerebral artery aneurysms. (A) very tortuous supra-arch vessels. (B) left VA angiogram in working projection revealed highly irregular multi-lobulated left PCA aneurysm. (C) 3D reconstruction demonstrated the complex topography of the aneurysm. There were multiple aneurysms with different diameters located from the origin of the left PCA to the conjunction of P1 and P2. (D) the microcatheter tip could not be advanced further beyond the origin of the largest aneurysm neck (the black arrow) over the microwire because of the extremely high tension at the acute turning point of P1(the white arrow). We kept the microcatheter tip at the aneurysm neck and inserted the coil. Some of the loops entered the distal sac of the aneurysm. (E) with the coil being held stable, the microcatheter was advanced until its tip got into the distal sac of the aneurysm. (F) and (G) the aneurysms were completely occluded with the embolization. (H) Follow-up 3D reconstruction after seven months demonstrated ongoing occlusion of the aneurysm.
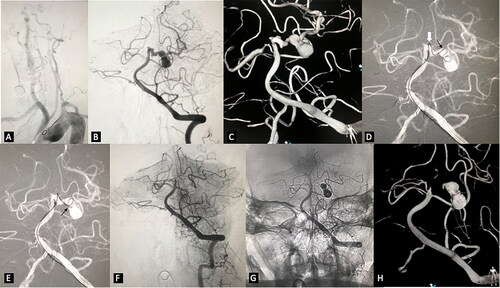
Figure 2. Right posterior communicating aneurysm was embolized with the novel coil guiding catheterization technique. (A) working projection revealed an irregular shaped aneurysm located in the posterior communicating artery segment. (B) 3D reconstruction demonstrated very tortuous vessel access. (C) the microcatheter tip was advanced near the aneurysm neck (small black arrow). The coil was inserted. Coil loops were protruded to the distal ICA and A1, some were in the aneurysm sac. (D) the microcatheter was advanced while the coil was slightly retrieved until the microcatheter tip was totally in the aneurysm sac. (E) the coil outside the aneurysm sac was retrieved before the true framing process started. (F) final control after the coiling demonstrated no contrast filling of the aneurysm sac.