Figures & data
Figure 1. STARD diagram depicting the study design and classification of study participants. The study participants were classified as definite TBM, probable TBM and no-TBM using a uniform research case definition (Marais et al. Citation2010). CRF: case report form; CSF: cerebrospinal fluid; ELISA: enzyme-linked immunosorbent assay; TBM: Tuberculous meningitis; no-TBM: children presenting with signs and symptoms suggestive of TBM, but finally diagnosed with other meningitis or no meningitis (see ).
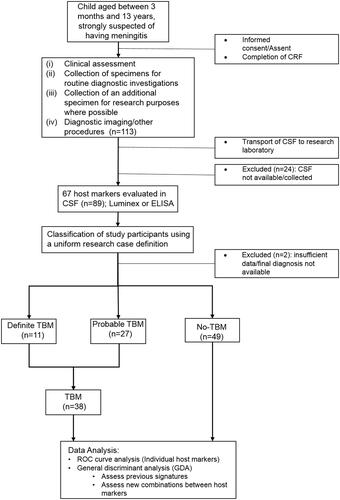
Table 1. Clinical and demographic characteristics of study participants.
Figure 2. Performance of the previously identified host CSF protein biosignatures in the diagnosis of TBM in children. Receiver operator characteristics (ROC) curve showing the accuracy of the three-marker CSF biosignature (VEGF + IFN-γ + MPO) (Manyelo et al. Citation2019a) in diagnosing TBM (A), Scatter plot showing the ability of the three-marker biosignature in discriminating between TBM and no-TBM (B), ROC curve showing the accuracy of the four-marker CSF biosignature (IFN-γ + MPO + ICAM-1 + IL-8) (Manyelo et al. Citation2019a) in diagnosing TBM (C), Scatter plot showing the ability of the four-marker biosignature in discriminating between TBM and no-TBM (D).
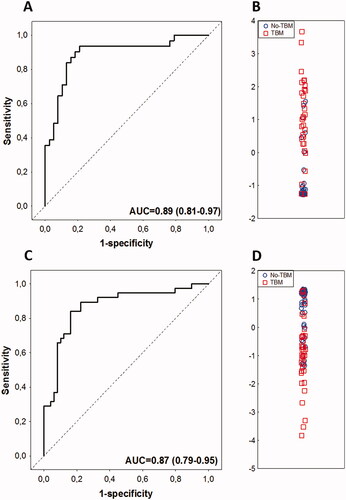
Table 2. Diagnostic accuracy of the host CSF protein biosignatures described in the present study in the diagnosis of TBM in children.
Table 3. The diagnostic accuracy obtained when the study participants were diagnosed as TBM based on data from one or more of the three proteins in the 3-marker signature (Manyelo et al. Citation2019a).
Table 4. The diagnostic accuracy obtained when the study participants were diagnosed as TBM based on data from one or more of the four proteins in the previously identified 4-marker signature (Manyelo et al. Citation2019a).
Figure 3. Scatter plots showing the concentrations of CCL1 (A), IFN-γ (B), TNF-α (C), VEGF-A (G), GM-CSF (H), and CXCL9 (I) in CSF samples from children with TBM and no-TBM, and the receiver operator characteristics curves showing the accuracies of CCL1 (D), IFN-γ (E), TNF-α (F), VEGF-A (J), GM-CSF (K), and CXCL9 (L) in the diagnosis of TBM. The error bars depict the median concentrations and interquartile ranges. Uncorrected Mann-Whitney U test p-values for the differences between the medians of the groups are shown for each biomarker. Data obtained after correcting for multiple testing are shown in and Supplementary Table 2. Representative plots for the six most accurate individual biomarkers (AUC > 0.90) are shown.
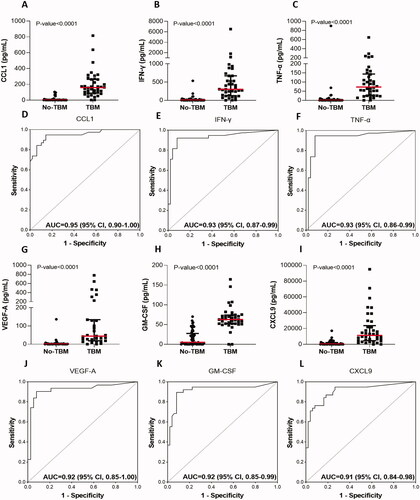
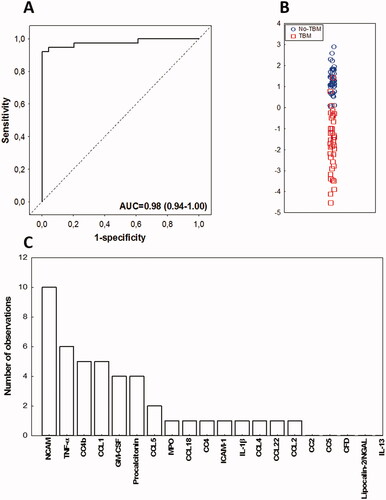
Figure 4. Performance of the alternative CSF protein biosignature in the diagnosis of TBM in children. Receiver operator characteristic (ROC) curve showing the accuracy of the novel four-marker CSF biosignature (CC4b + CC4 + Procalcitonin + CCL1) in the diagnosing TBM (A), Scatter plot showing the ability of the four-marker biosignature in discriminating between TBM and no-TBM (B), Frequency of proteins in the top 20 general discriminant analysis (GDA) models that accurately classified children with TBM and no-TBM (C).