
Figures & data
Figure 1. Model structure. Patient enters the model at the top, to start in a pathway tree of max four cycles, where patient can go between visit to specialist, conservative care, and inpatient care. If patient enters surgery, he goes into Markov post-surgical care (MPSC). Otherwise, patient enters Markov non-surgical care (MNSC) or dies at any stage in the model.
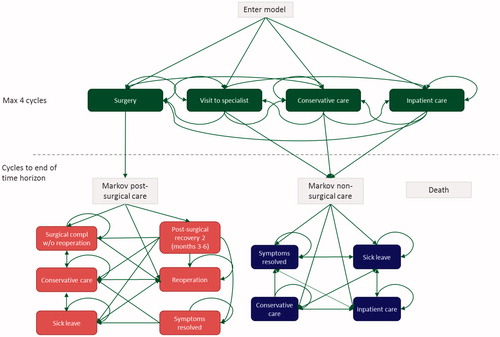
Table 1. Definitions of states in the model. States lower in the table take precedence, so that, for patients fulfilling conditions for two or more states simultaneously, the state lower in the table is chosen.
Table 2. Patient characteristics.
Table 3. Average cost and accrued quality adjusted life years (QALYs) and life years, averaged over the whole patient population. QALYs lost are calculated as difference from normal population. All values are discounted.
Figure 2. Sensitivity analysis of total societal burden by level of willingness-to-pay (WTP) used for the valuation of QALYs. Base case WTP is set at €70,000.
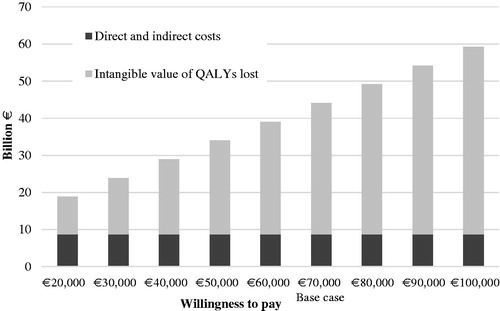
Table 4. Results of sub-group analyses, discounted values. Total costs include direct (outpatient/inpatient visits, pharmaceuticals, surgery) and indirect costs (productivity cost due to work absence), but exclude intangible costs in terms of monetary value of lost QALYs.