Figures & data
Table 1. Baseline patient demographic and clinical characteristics.
Figure 1. Markov model for HK in CKD patients with or without HF. The squares represent different health states that are mutually exclusive. CKD stages 3–4 and NHYA I–IV represent starting health states. Abbreviations. CKD, chronic kidney disease; HF, heart failure; HK, hyperkalemia; MACE, major adverse cardiac events; NYHA, New York Heart Association; RAASi, renin-angiotensin-aldosterone system inhibitors.
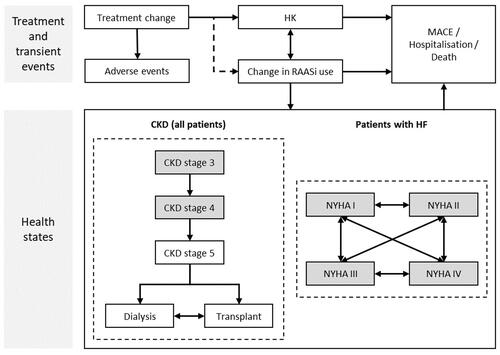
Table 2. Costs and utilities included.
Table 3. Base case and one-way scenario analyses results: patiromer vs. no patiromer (€2021).
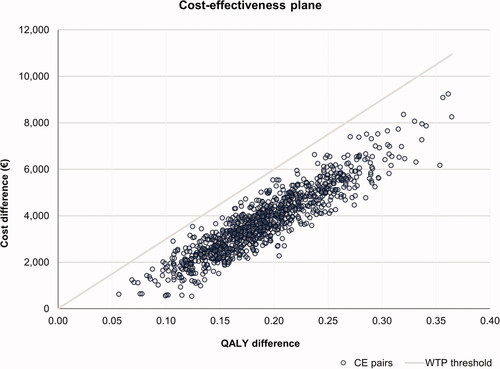
Figure 2. Cost-effectiveness plane for patiromer versus no patiromer. A WTP threshold of €30,000 per QALY gained was assumed. Abbreviations. CE, cost-effectiveness; QALY, quality-adjusted life-years; WTP, willingness-to-pay.