
Figures & data
Figure 1. (a) Types of aortic dissection according to the Stanford classification system (shown at top) and the DeBakey classification system (shown at bottom). (b) Intimal tear and propagation of the dissection between the media and intima layers of the ascending aorta. Drawings: Hjördís Bjartmarz. Copyright ©Tomas Gudbjartsson.
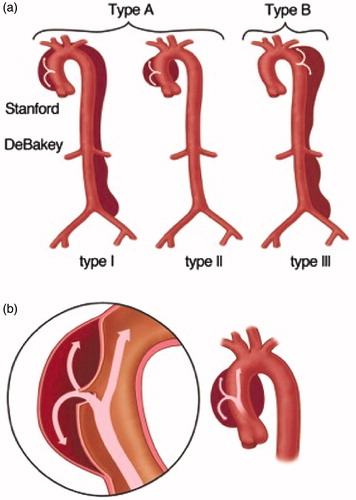
Table 1. Major risk factors for aortic dissection.
Figure 2. (a) Acute type-A dissection seen intraoperatively with typical appearance where blood can be visualized underneath a thinned out adventitia of the ascending aorta. (b) Preoperative CT scan of the same patient. Photos: Tómas Gudbjartsson.
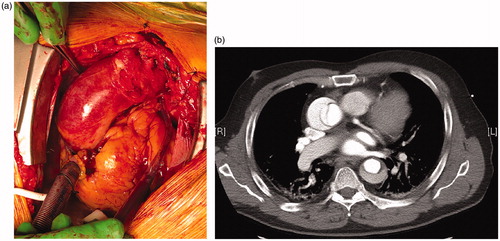
Figure 3. (a) Malperfusion of the kidneys in a patient with ATAAD. The left kidney has delayed enhancement of contrast through the false lumen of the dissection while the right renal artery has normal perfusion from the true lumen. Photo: Tómas Gudbjartsson. (b) Type A dissection stretching from the aortic root and into the brachiocephalic trunk and causing stroke due to carotid malperfusion. The intimal tear is seen with a complex dissection flap which divides the vessels into a true and false lumen. Photo: Arnar Geirsson. (c) The pathology of pericardial tamponade in ATTAD with an intimal tear in the aortic root. Drawing: Hjördís Bjartmarz. Copyright: ©Tomas Gudbjartsson.
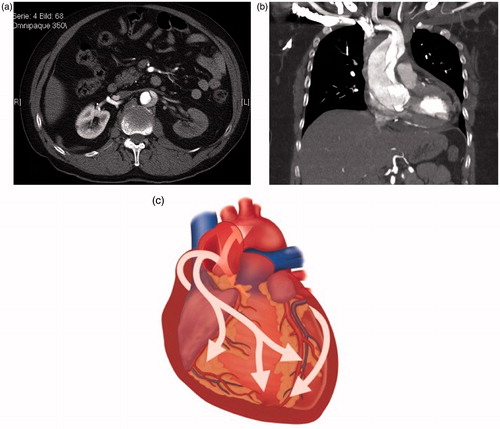
Figure 4. Key steps in surgical repair of ATAAD. (a) Resection of the ascending aorta starting proximally at the sinotubular junction. (b) Resuspension of the aortic valve commisures to treat or prevent aortic regurgitation. (c) Open distal anastomosis with hemiarch replacement (with perfusion cannulae omitted for clarity). (d) Completed repair; perfusion through integrated graft side-arm. Drawings: Hjördís Bjartmarz. Copyritght: ©Tomas Gudbjartsson.
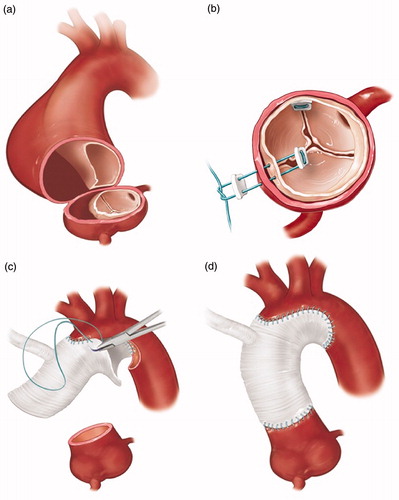
Table 2. Postoperative complications following ATAAD repair as reported from the NORCAAD registry.
Table 3. Major predictors of 30-day and long-term mortality in ATAAD patients.