Figures & data
Figure 1. Flow chart of patient inclusion and exclusion. Patients were excluded in a stepwise process.
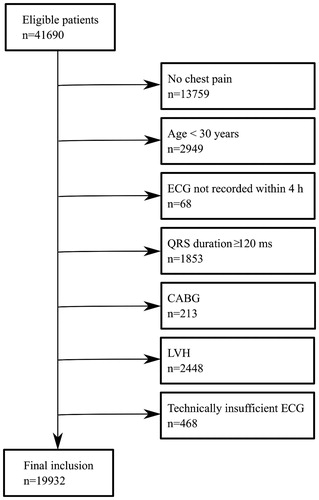
Figure 2. Explanation and basis of the extended STEMI criteria. Limb leads (to the left) and chest leads (to the right) presented in anatomical context.
Left image: The inverted version of lead III (–III) is contiguous and presented adjacently to aVL, the inverted version of aVL (–aVL) is contiguous to lead III, and the inverted version of lead I (–I) is contiguous to both –aVL and aVR. The inverse of aVR (–aVR) is contiguous to lead I and lead II. In this purely illustrative example, significant ST elevation is present in only one of the conventional leads (lead III), but in two contiguous leads when the extended STEMI criteria are applied (III and –aVL).
Right image: In the extended STEMI criteria, the inversion of leads V1, V2 and V3 (–V1, –V2, –V3) are also included in order to cover the lateral aspects of the left ventricle. ECG shows ST depression in V1 – V3, which is equivalent to ST elevation in –V1, –V2 and –V3.
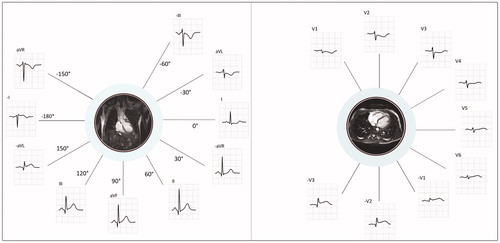
Table 1. Patient characteristics.
Table 2. Outcomes for patients meeting and not meeting STEMI criteria.
Table 3. Diagnostic accuracy of conventional and extended STEMI criteria.
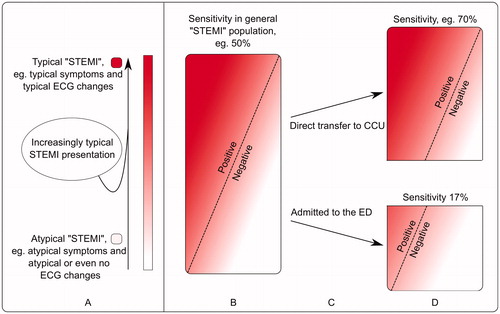
Figure 3. Schematic explanation of how sensitivity of STEMI criteria is affected in different populations.
Although sensitivity and specificity are not related to the prevalence of disease (as opposed to PPV and NPV), they can still be affected by a difference in attributes of the patients.
A. The entire population of patients with acute coronary occlusion is heterogeneous and patients may present with either typical ECG changes and typical symptoms on one end of the spectrum, or with atypical symptoms and atypical ECG changes on the other. In this illustration, patients with typical presentation are represented by an intense red color and patients with atypical presentation represented by pink/white colors.
B: The rectangle represents all patients with acute coronary occlusion – here referred to as the general “STEMI” population. STEMI criteria have been assigned a hypothetical sensitivity, 50%, for the detection of acute coronary occlusion. Patients to the left of the dashed line meet STEMI criteria (positive), while patients to the right of the dashed line do not (negative).
C: Patients with typical symptoms and/or typical ECG changes (more red) are more likely to be directed to the coronary care unit (CCU) than those with atypical presentation (pink/white), who instead are more likely to present at the emergency department (ED).
D: Since atypical ECG changes are more common among those patients who present at the ED, STEMI criteria will not detect as many patients with acute coronary occlusion as in the population in B, i.e. sensitivity decreases.