
Figures & data
Figure 1. Radiographic findings. (a–c) Seventy-three-year-old man with IgG4-related periaortitis. (a) Precontrast CT shows the soft tissue density mass around the abdominal aorta (white arrows). (b) The arterial phase of dynamic contrast-enhanced CT shows the inferior mesenteric artery in the soft tissue density mass (thin arrow). The atherosclerotic plaque is not enhanced (arrowheads). (c) The delayed phase of dynamic contrast-enhanced CT shows that the periaortic mass is slightly enhanced (arrows). A high density thin layer is seen between the atherosclerotic plaque and the periaortic mass (small arrows). (d,e) A 68-year-old man with IgG4-related periarteritis. (d) The arterial phase of dynamic contrast-enhanced CT shows a soft tissue density mass around the left common carotid artery (arrows). (e) The delayed phase of dynamic contrast-enhanced CT shows that the mass is slightly enhanced (arrows). Stenosis of the left common carotid artery is not seen in this case. (f,g) A 63-year-old man with IgG4-related periarteritis. (f) The arterial phase of dynamic contrast-enhanced CT shows a soft tissue density mass around the inferior mesenteric artery (arrows) with a luminal stenosis (thin arrow) and calcification (small arrow). (g) In the reconstructed sagittal image, the luminal stenosis can be clearly seen (thin arrow). (h–i) IgG4-related abdominal inflammatory aneurysm treated by stent graft implantation.
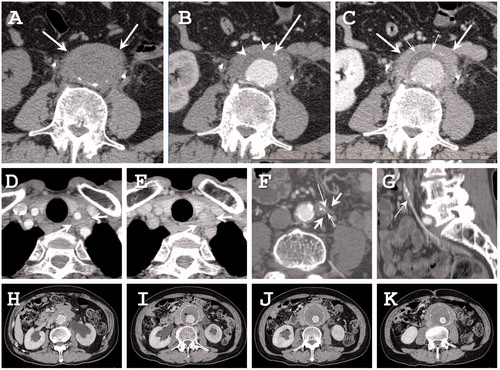
Figure 2. Histopathological findings of IgG4-related abdominal aortic aneurysm. (a) Inflammation with lymphoplasmacytes is observed predominantly in the medial layer. (b) Diffuse inflammation with lymphoid follicles and fibrosis are detected mainly in the adventitia layer that is in part spreading to adjacent adipose tissue. (c) Fibrosis progresses to adjacent adipose tissue. (d,e) Massive infiltration of IgG4-immunopositive cells in adventitia (d and e correspond to box areas of a and b, respectively). (f) Perineural infiltration. (g) storiform fibrosis. A higher magnification of the box area of (c). Original magnifications and scale bar, respectively, are ×12.5 and 500 μm (a–c), ×200 and 50 μm (d, e), and ×100, and 100 μm (f, g). i, intima; m, media; a; adventitia.
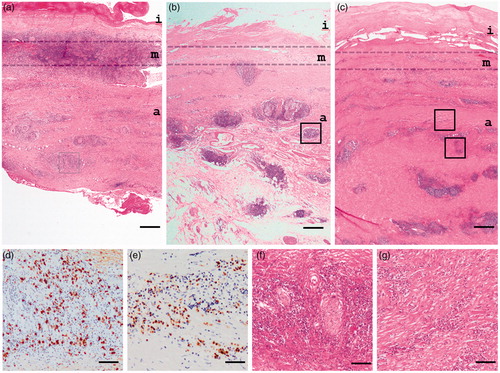
Table 1. Diagnostic criteria for IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis.