Figures & data
Figure 1. (A) Diffusion tensor imaging (DTI) tractography models diffusion of water at each voxel using a tensor model, characterized by 3 orthogonal eigenvectors and their corresponding eigenvalues (λ1, λ2, λ3). The principal diffusion direction is the eigenvector with the largest eigenvalue, λ1, in this example. (B) Streamline tractography traces the principal diffusion directions of tensors through adjacent voxels to estimate underlying white matter tracts in 3-dimensional space.
Figure 2. Tractography for subcallosal cingulate cortex (SCC) DBS. Effective SCC DBS involves concurrent stimulation of 4 white matter tracts: the forceps minor (red), the uncinate fasciculus (purple), the cingulum bundle (yellow), and the fronto-striatal fibres (not shown). These white matter tracts are used to guide lead placement for SCC DBS.
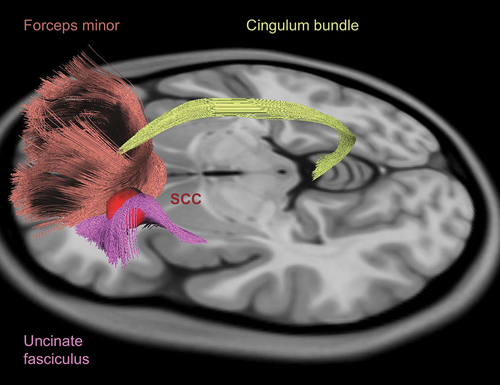
Figure 3. Tractography for ventral tegmental area projection pathway (VTApp) DBS. Lead placement for VTApp DBS is primarily guided by tractography. The target is the VTApp (orange) as it exits the ventral tegmental area (VTA) (green), bordered by the subthalamic nucleus (STN) (light purple) and substantia nigra pars reticulate (SNr) (dark purple) laterally, the red nucleus posteriorly (not shown), and the mammillary body anteriorly (not shown).
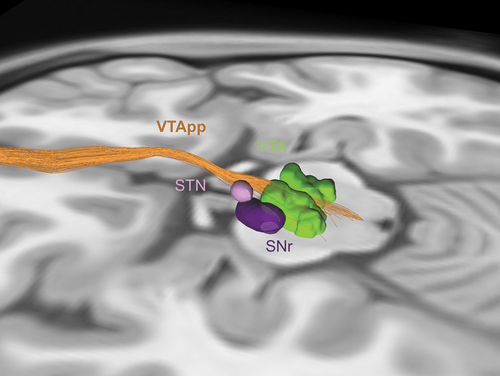
Figure 4. Tractography for ventral capsule/ventral striatum (VC/VS) and bed nucleus of the stria terminalis (BNST) DBS. VC/VS and BNST DBS are currently performed using stereotactic coordinates to target the NAcc (blue) and BNST (red) respectively, with the lead passing through the internal capsule. These targets are in close proximity to each other and to white matter tracts associated with depression-related networks, such as the ventral tegmental area projection pathway (VTApp) (orange) and anterior thalamic radiation (ATR) (purple). As such, there is potential for tractography to guide lead placement in this region.
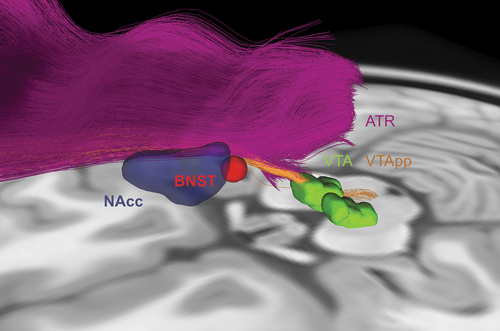
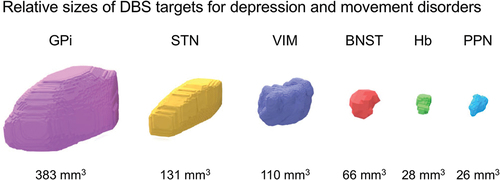
Figure 5. Size comparison of nuclear DBS targets for treatment-resistant depression (TRD) and movement disorders. Estimated volumes vary based on the source atlas, methodology, and neuropathology. In addition, volumes gradually decrease with normal aging and neurodegenerative diseases. Smaller nuclei are more challenging to target for DBS. In TRD, the identification of the bed nucleus of the stria terminalis (BNST) and habenula (Hb) is aided by high-resolution structural MRI. Of note, these nuclei are small relative to the size of a DBS lead and potential volume of tissue activated. GPi, globus pallidus interna; STN, subthalamic nucleus; VIM, ventral intermediate nucleus of the thalamus; PPN, pedunculopontine nucleus.