
Figures & data
Figure 1. Representative computed tomography (CT) scans at thoracic level used to determine muscle area in chronic obstructive pulmonary disease (COPD). (A) CT image used for pectoralis muscle imaging shaded in light blue. (B) CT image for erector spinae muscle imaging shaded in light blue. Label delineates the designated Hounsfield units for skeletal muscle from –50 to 90, the percentage of skeletal muscle mass, and the CSA measured in cm2.
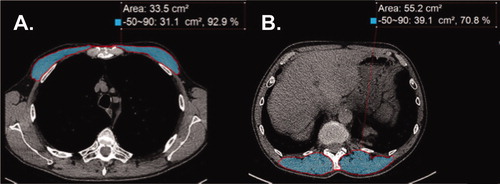
Table 1. Baseline clinical and demographic characteristics of lung cancer screening (LCS) control subjects and chronic obstructive pulmonary disease (COPD) case subjects.
Table 2. Clinical characteristics of patients with COPD.
Table 3. Spirometric measures and AATD testing of patients with COPD.
Figure 2. Muscle area in COPD patients and smoking controls. (A) Distribution of pectoralis muscle area (in cm2) stratified by GOLD stage compared to current and former smoking controls. †<p < 0.01, ‡p < 0.05 for Tukey’s test for intergroup differences. (B) Distribution of erector spinae muscle area (in cm2) stratified by GOLD stage compared to current and former smoking controls. Tukey’s test did not show significant intergroup differences.
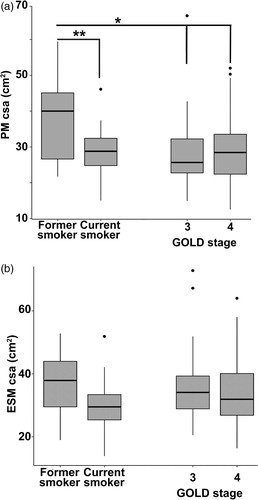
Table 4. Bivariate assessment of covariates with pectoralis muscle (PM) area in COPD subjects.
Table 5. Bivariate assessment of covariates with Erector Spinae muscle (ESM) area in COPD subjects.
Table 6. Relationship between PM CSA and physiologic parameters/clinical traits.
Table 7. Relationship between ESM CSA and physiologic parameters/clinical traits.
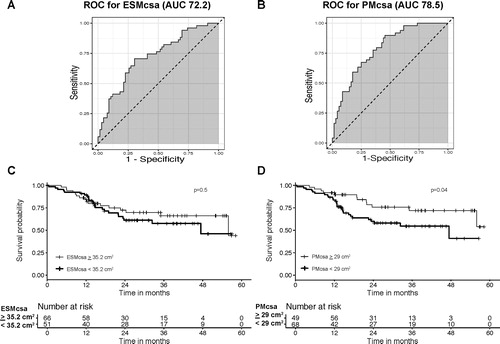
Figure 3. Survival analysis of patients with COPD. (A) and (B) Receiver operating characteristic curves to determine the optimum cutoff value for ESM and PM CSA and the event (death, bronchoscopic or surgical lung volume reduction surgery, or lung transplant). Area under the curve was 72.2 for ESM CSA and 78.5 for PM CSA. (C) Kaplan–Meier survival curves stratified by ESM CSA. The cutoff value corresponds to greater than or equal to the mean ESM CSA and less than the mean ESM CSA (≥ 35.2 cm2 and <35.2 cm2, respectively). The solid line indicates event-free survival probability. The crosses indicate censoring. The steps down indicate events (mortality, lung volume reduction surgery, or lung transplant). There was no significant difference for patients with COPD who had lower ESM CSA values in terms of event-free rates (p = 0.5 by log rank test). (D) Kaplan–Meier survival curves stratified by PM CSA. The cutoff value corresponds to greater than or equal to the mean PM CSA and less than the mean PM CSA (≥ 29 cm2 and <29 cm2, respectively). The solid line indicates event-free survival probability. The crosses indicate censoring. The steps down indicate events. The patients with COPD and lower PM CSA values exhibited significantly worse event-free rates (p = 0.04 by log rank test).
Data availability statement
A data availability statement provided by the authors is available upon request.