Figures & data
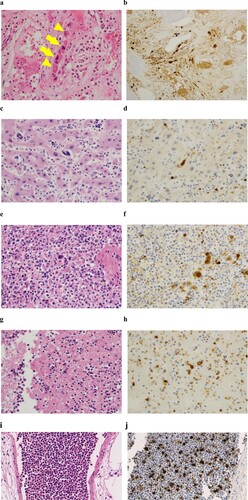
Figure 1. Bone marrow histology in low-power (a and c; x100) or high-power (b and d ∼ h; x400) fields at diagnosis (a ∼ d), transformation into fibrosis (e and g) and the exaggerated thrombocytosis phase (f and h). a, b: H-E staining revealed slightly hyperplastic bone marrow with an increased number of dysplastic megakaryocytes. Two distinct types of dysplastic megakaryocytes were observed. One type exhibited abundant and mature cytoplasm and deeply and hyperlobulated nuclei (staghorn-like), whereas the other type exhibited an altered nuclear:cytoplasmic ratio with abnormal chromatin clumping and plump (cloud-like) or bulbous (balloon-shaped) lobulation of the nuclei. These two types of abnormal megakaryocytes formed loose clusters. Arrows and arrowheads indicate abnormal megakaryocytes with staghorn-like and cloud-like nuclei, respectively. c, d: Silver staining of the initial bone marrow biopsy revealed a very loose network of reticulin fibre, and the condition was categorized as grade 0 myelofibrosis (MF-0) based on the criteria of the European consensus on grading bone marrow fibrosis. e, f: H-E staining revealed infiltration of dysplastic megakaryocytes in the secondary (e) and tertiary (f) analyses. g, h: Silver staining of the secondary (g) and tertiary (h) bone marrow biopsy revealed obvious fibrosis. Compared with the secondary biopsy (g), the tertiary sample (h) exhibited more prominent fibrosis.
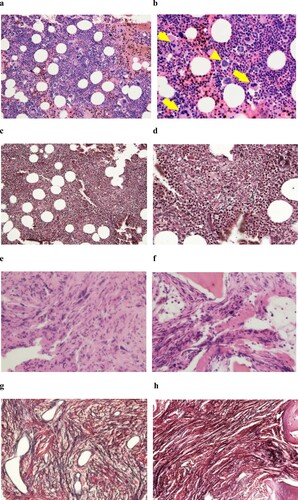
Figure 2. Clinical course.
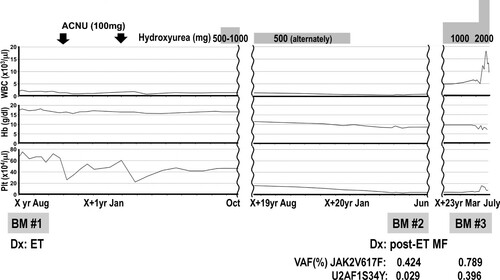
Table 1. Laboratory findings.
Figure 3. H-E staining of the bone marrow (a), liver (c), spleen (e), thrombus (g) and lung (i) at autopsy. Infiltration of dysplastic megakaryocytes was confirmed with anti-CD42b immunostaining in the bone marrow (b), liver (d), spleen (f), thrombus (h) and lung (j). Arrows and arrowheads indicate abnormal megakaryocytes with staghorn-like and cloud-like nuclei, respectively (a).