Figures & data
Figure 1. (a) A 55 mm abdominal aortic aneurysm with short neck (average diameters of 27.6 mm and 32.7 mm at 7 mm at 10 mm diameter below the lowermost renal artery, respectively). (b). Efficient sealing relies on the accurate apposition of the first sealing ring immediately below the renal arteries. (c). Intraoperative completion angiography demonstrating technical success, i.e. aneurysm exclusion without endoleak (image courtesy of Dr. Kapoulas).
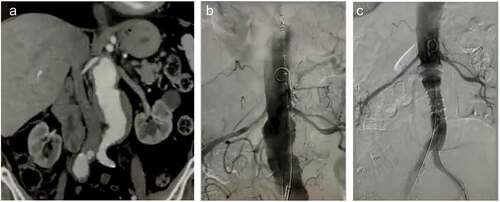
Figure 2. (a). A 52 mm abdominal aortic aneurysm with conical neck (diameters of 21.7 mm and 24 mm at 7 mm at 10 mm diameter below the lowermost renal artery, respectively). (b). Efficient sealing relies on the adjusted apposition on the conical irregularities of the neck. (c). The balloon is slightly advanced 5–7 mm cranially to inflate and facilitate accurate sealing (image courtesy of Dr. Georgakarakos).
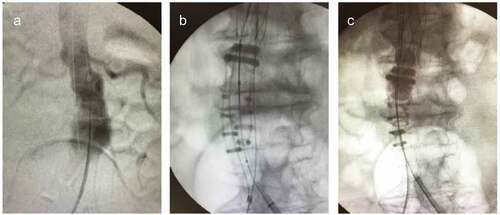
Figure 3. (a). A 55 mm juxtarenal Abdominal Aortic aneurysm in a 70 year-old female patient ineligible to sustain open repair or complex endovascular solution. (b). The outer-to-outer wall of the infrarenal neck wall reaches a maximum diameter of 37 mm at 7 mm infrarenally. (c). Yet, the lumen diameter differs significantly from the outer diameter, estimated 19–25 mm. (d). An Ovation Alto achieved successful sealing in the distended neck, deployed actually within the aneurysm. The arrows depict the transition of the aneurysm extending proximally to the infrarenal level. (e). Absence of endoleaks confirmed 1-month postoperatively in computed tomography with intravenous contrast. (f). The landing of the radiopaque polymer-filled ring within the lumen against the burden of the thrombus surface in the non-contrast computed tomography (image courtesy of Dr. Georgakarakos).
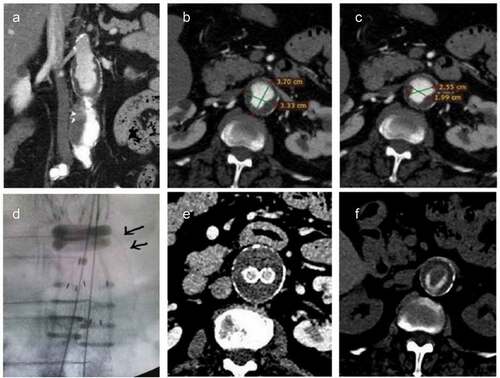
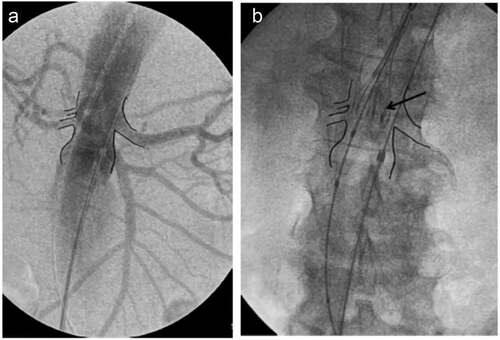
Figure 4. (a). Intraoperative angiography of an aneurysm to mark the orifice of the renal arteries. (b). In order to achieve very precise sealing at 7 mm infrarenally, it is advisable to begin deployment with the proximal markers (arrow) of the top end of the graft aggressively at the level of the renal arteries – or even more centrally- in order to counterbalance an anticipated small caudal migration upon completion of the deployment (image courtesy of Dr. Georgiadis).