Figures & data
Figure 1. The effects and blockade of interleukin 6 signaling.
The effects of interleukin 6 (IL-6) are mediated via two main signaling pathways. The ‘classical’ signaling pathway (green boxes) is associated with the homeostatic effects of the cytokine and involves cell types expressing the IL-6 receptor (IL-6) on their cell membrane. The ‘trans’ signaling pathway (red boxes) mediates effects via most cell types (i.e., all cells that express gp130 on their membrane) and is associated with inflammation-related pathologies and diseases such as rheumatoid arthritis and, according to current preliminary evidence, cardiometabolic diseases including diabetes, cardiovascular disease and chronic kidney disease. IL-6 ‘trans’ signaling requires shedding of the IL-6 R into its soluble form (sIL-6 R); the membrane metalloprotease ADAM17 (and/or ADAM10) is responsible for the cleavage of the IL-6 R. More details are available in the text. Anti-IL-6 compounds (blue boxes) target the IL-6 cytokine to interfere with its binding to the IL-6 R and gp130 receptor complex, whilst anti-IL-6 R agents block the IL-6 R; both these interventions block the ‘classical’ and ‘trans’ signaling pathways. One compound (sgp130Fc) is currently in development to block the ‘trans’ signaling pathway exclusively. Finally, blockers of intracellular STAT and JAK factors also are available to block the actions of IL-6 following activation of the IL-6 R/gp130 complex.
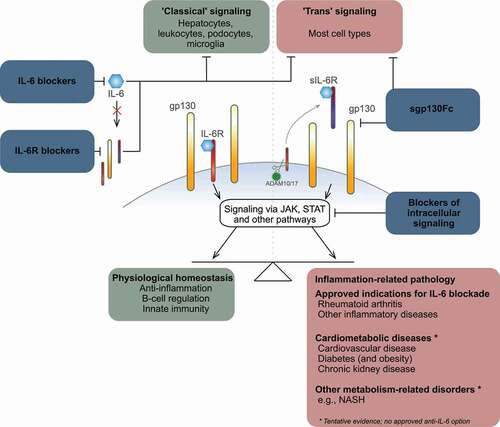
Table 1. Licensed and selected in-development blockers of interleukin 6 signaling
Figure 2. Interleukin 6 in cardiometabolic disorders.
Chronic inflammation, including elevated levels of interleukin 6 (IL-6), is associated with diabetes, cardiovascular disease and chronic kidney disease, as well as related diseases such as nonalcoholic hepatosteatosis. Amongst other triggers, elevated IL-6 levels may arise due to excess adipose tissue and can cause, for example, aberrant glucose metabolism leading to diabetes and other manifestations of the ensuing glucotoxicity in many tissues and organs, including the vasculature and other parts of the heart and the kidneys, as well as in the liver. IL-6 is also associated with atherosclerosis and cardiovascular disease and chronic kidney disease. The illustration is not exhaustive and is a simplistic, IL-6-centric representation of the complex interplay between the cardiometabolic diseases.
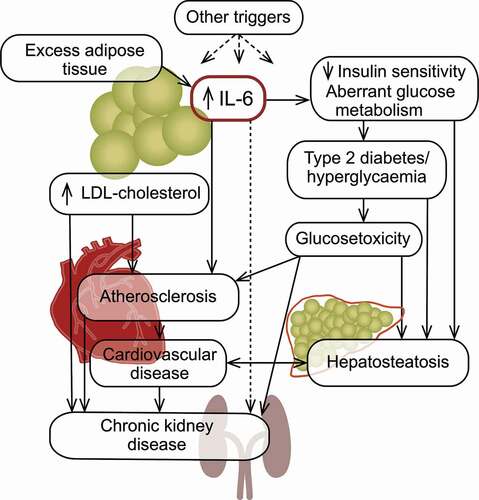
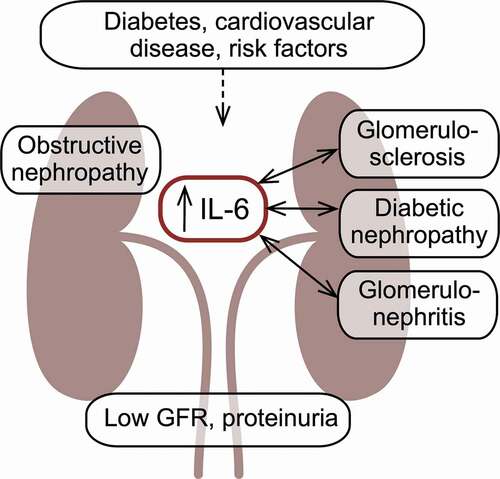
Figure 3. Interleukin 6 in chronic kidney disease.
Chronic kidney disease due to diabetic nephropathy, glomerulosclerosis or glomerulonephritis is associated with elevated levels of interleukin 6. Studies are needed to clarify the exact role of the cytokine in the disease and whether the elevated levels constitutes a pathogenic trigger or a manifestation of, for example, reduced renal clearance of the cytokine due to the reduced glomerular filtration function associated with renal impairment.