Figures & data
Figure 1. Both rotational (left) and hinge (center) knee prostheses, optionally furnished with patella flange (right). Flexion and rotation of the rotational knee prosthesis take place in a cross-joint. A connecting piece, which is fixed to the tibial component and links it to the femoral component of the hinge knee prosthesis, features a borehole for the joint axis.
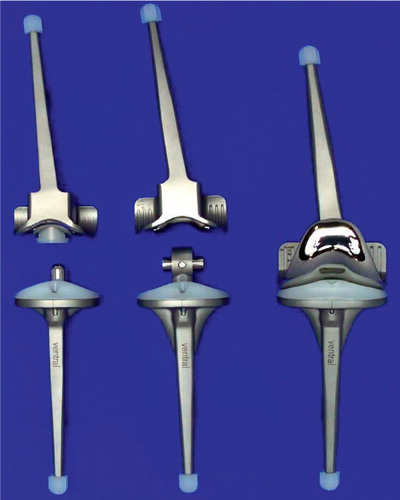
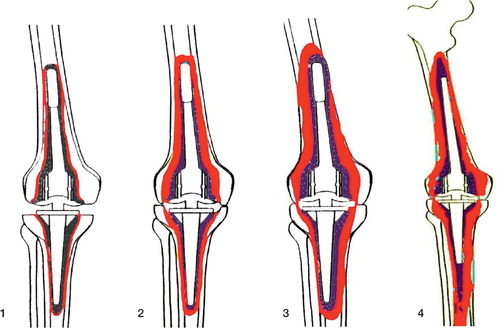
Figure 2. ENDO classification (Engelbrecht Citation1993) with regard to constrained knee prostheses: increasing loss of bone stock (colored red) from type 1 to type 4. Type-1 defects are minor bone defects with thin radiolucent lines but no subsidence of components. Type-2 defects involve moderate bone loss, evidenced by wider radiolucent lines around the entire implant and clear signs of subsidence. Depending on the model used, there may be thinning of the distal femoral or tibial proximal cortex or of the cancellous bone within the region of the femoral and tibial condyles. Type-3 defects are severe loss of bone with widening of the distal femur or proximal tibia, cortical thinning with perforations, and severe condylar defects. Type-4 defects are massive: there is total or severe loss of bone stock. More than half of the femur is defective, or the remains of the middle or proximal parts are weakened by severe cortical thinning or severe osteoporosis from lack of use.
Radiographic assessment of bone graft incorporation
Figure 3. Postoperative control after IBG reconstruction of the femoral cavity in patient A, who had a type-3 defect.

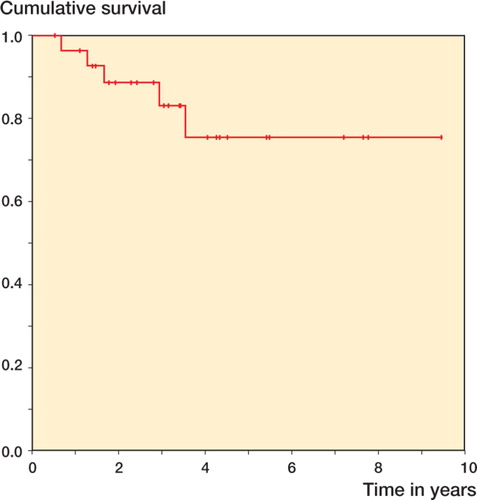
Figure 4. Kaplan-Meier survivorship. The endpoint used was: any part of the prosthesis removed or revised for any reason.