
Figures & data
Table 1. The characteristics of the 7 patients with a flexion-type supracondylar humerus fracture
Figure 1. The primary radiographs (anterior-posterior and lateral projection) of all flexion-type supracondylar humerus fractures (cases I–VII) during the 10 years of the study period (2000–2009). Postoperative radiographs and the radiographs at the last short-term follow-up visit are also presented.
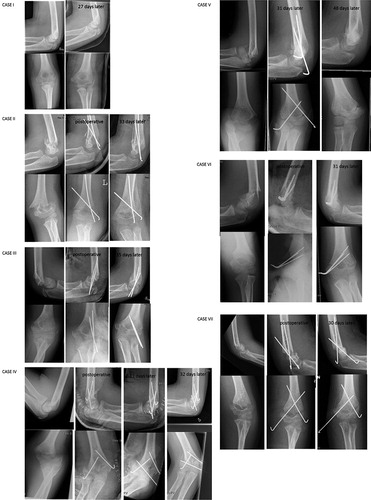
Figure 2. A radiographic investigation (antero-posterior and lateral projections) of the elbow showing an increased carrying angle 9 years after the injury. The patient (case IV) was 14 years old when he sustained a Gartland-Wilkins type-IV supracondylar humerus fracture.
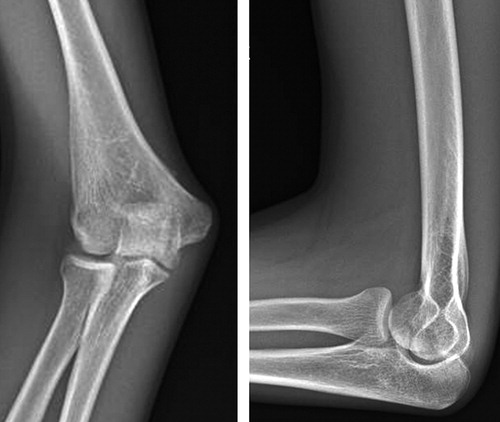
Table 2. Long-term clinical recovery of flexion-type supracondylar humerus fractures mean 9 (5–11) years after the injury
Table 3. Outcome measurements for the patients with a former flexion-type supracondylar humerus fracture mean 9 years after the injury
Table 4. Patient demographics, fracture classification, and treatment of flexion-type supracondylar fractures in children according to the current study and the literature available since 1990