
Figures & data
Figure 1. Flow chart for patients included in the study.
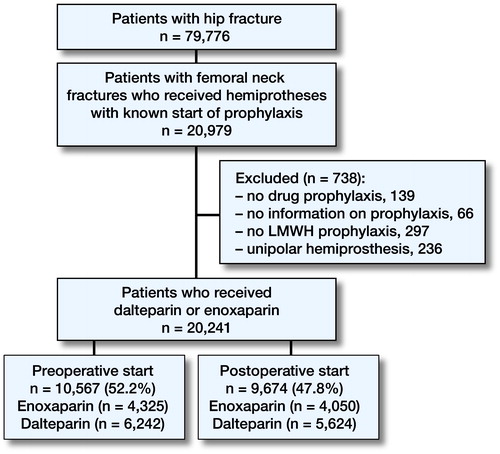
Figure 2. The timeline demonstrates the development in start of thromboprophylaxis from 2005–2014 for the patients observed in the study. Femoral neck fractures treated with bipolar hemiarthroplasty with known start of thromboprophylaxis (dalteparin or enoxaparin).
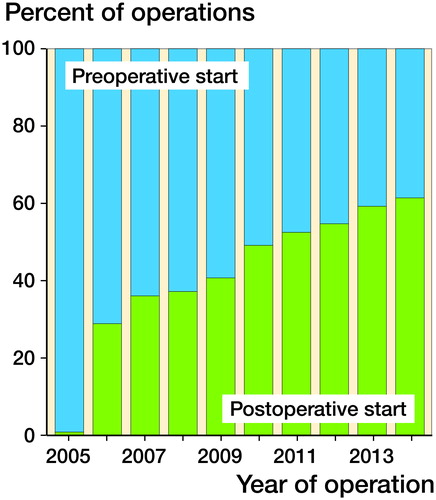
Figure 3. Postoperative mortality and risk of reoperation for patients with femoral neck fractures treated with hemiprostheses.
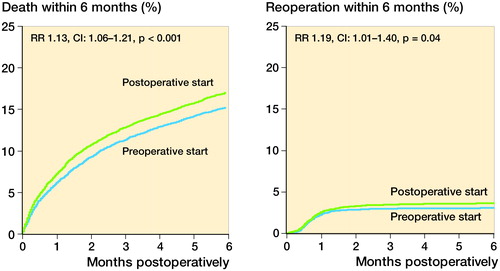
Table 1. Baseline characteristics of the patients/operations
Table 2. Mortality and risk of reoperation 7 days, 30 days and 180 days postoperatively after bipolar hemiarthroplasty due to femoral neck fractures. Cox relative risk ratio (RR) (with preoperative start of prophylaxis as reference) is given with adjustments for possible infl uences of sex, ASA-class, age of the patient at surgery, type of surgery, duration of surgery and year of surgery
Table 3. Mortality and risk of reoperation 180 days postoperatively in patients receiving an uncemented and cemented hemiarthroplasty (HA). Cox relative risk ratio (RR) (with preoperative start of prophylaxis as reference) is given with adjustments for possible influences of sex, ASA-class, age of the patient at surgery, duration of surgery and year of surgery
Table 4. Effect of postoperative start of thromboprophylaxis versus preoperative start 180 days postoperatively in healthy patients (ASA 1-2) and in morbid patients (ASA 3-5) with femoral neck fracture operated with bipolar hemiprosthesis. Cox relative risk ratio (RR) (with preoperative start of prophylaxis as reference) is given with adjustments for possible influences of sex, age of the patient at surgery, type of surgery, duration of surgery and year of surgery
Table 5. Mortality and risk of reoperation 180 days postoperatively in patients operated with hemiprosthesis with a preoperative start of thromboprophylaxis (n= 9,370) where the primary dose was of full standard (5 000 IU dalteparin or 40 mg enoxaparin) or half standard (2 500 IU dalteparin or 20 mg enoxaparin) dosage. Cox relative risk ratio (RR) (with full dose at start of prophylaxis as reference) is given with adjustments for possible influences of sex, ASA-class, age of the patient at surgery, type of surgery, duration of surgery and year of surgery