Figures & data
Figure 1. A and B.The trimalleolar ankle fracture following closed reduction at the emergency department. C. Computed tomography revealing the extent of the posterior malleolar fracture. D and E. Intraoperative fluoroscopic images.
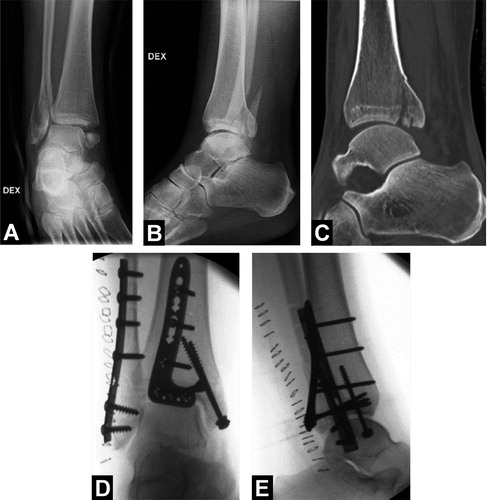
Figure 2. Computed tomography angiography revealing a vascular anomaly where a bilateral dominant peroneal artery was the only artery supplying vascularity to the foot.

Figure 3. Angiography showing occlusion of the peroneal artery at the level of the tip of the posterior plate (white arrows). Despite efforts to dissolve the occlusion with catheter-directed thrombolysis, the artery kept clotting.
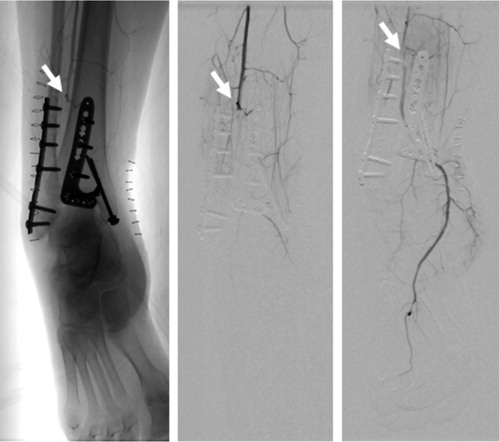
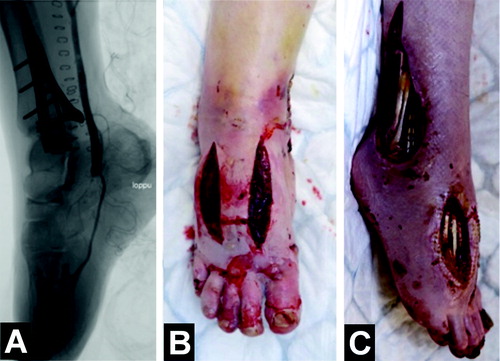
Figure 4. A. Occlusion of the peroneal artery was bypassed with a vein graft, and control angiography of the bypass graft showed blood flow to the plantar and digital arteries. B. Fasciotomies were performed due to the risk of compartment syndrome following revascularization. C. Despite the bypass, the patient developed severe ischemic damage, resulting in persistent foot pain and extensive soft tissue necrosis.