Figures & data
Figure 1. Flowchart of patient selection. a Residual and relapsed clubfeet.
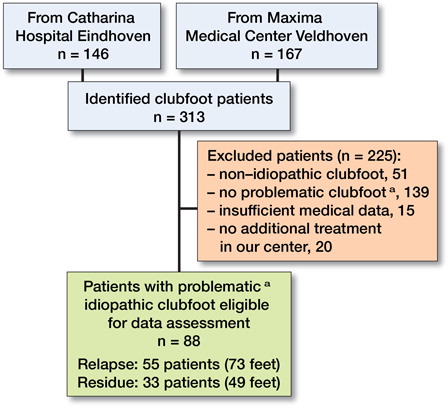
Table 1. Descriptive data on both groups for patients and feet
Table 2. Proportions of profiles of deformities in the relapse and residue group. Values are number of feet
Figure 2. Age at identification of the residual and relapsed clubfoot compared to the group of profiles of deformities in the clubfoot. Blue bars show the feet with solitary equinus and/or decreased dorsiflexion and green bars are those with other solitary deformities. Red bars indicate feet with combined profiles that contain EqDD and purple bars show feet with other combined profiles. Plain tones show patients that were referred to our clinic.
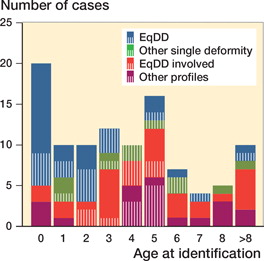
Figure 3. Age at identification of residual and relapsed clubfoot compared with their treatment group. Blue bars represent patients that had satisfying results with the Ponseti protocol. For patients displayed by green bars the Ponseti protocol was not sufficient and adaptation to a bracing protocol was needed to get good results. The red group contains those patients in which the previous 2 treatment options did not suffice and additive surgery was needed. Plain toned bars contain patients that were referred to our clinic.
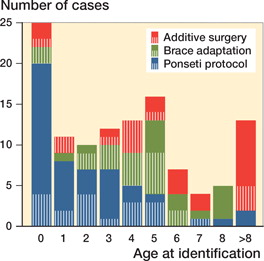
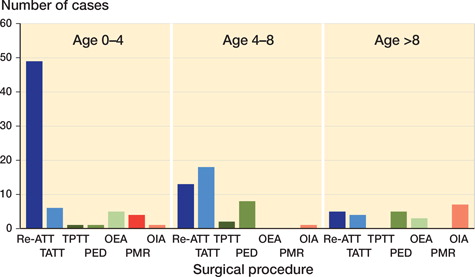
Figure 4. Age of patients at the moment of surgical intervention. Blue color marks the surgical treatments that are part of the Ponseti protocol. Green portrays extra-articular (EA) treatments that are not part of the Ponseti protocol. The red bars show the intra-articular (IA) treatments. Re-ATT: renewed Achilles tendon tenotomy, TATT: tibialis anterior tendon transfer, TPTT: tibialis posterior tendon transfer, PED: partial epiphysiodesis of the ventral distal tibia, OEA: other extra-articular surgery, PMR: posteromedial release, OIA: other intra-articular surgery.