Figures & data
Table 1. Etiology of LLD and treatment methods
Table 2. Outcome measures (mean and range values) of achieved lengthening and alignment, including unintentionally induced malalignment
Figure 1 20-year-old woman with CFD and fibular hemimelia. Initial shortening and valgus in the femur and valgus in the tibia. Femoral valgus and shortening were corrected with the retrograde nail technique; some remaining knee valgus due to deformity in the tibia. However, acceptable mechanical axis and currently no further surgery required. High-riding trochanter, but no Trendelenburg gait.

Figure 2 11-year-old girl with cerebral paresis and hemiplegia on her left side. Initial leg length discrepancy was 3 cm, where the hemiplegic side was the longer extremity. She had serious gait problems and gait analysis with shoe augmentation of 4 cm on the right side showed significant improvement of gait parameters. The girl was lengthened 4 cm in her right femur, overcorrecting her by 1 cm, which was advantageous with respect to her left-sided hemiplegia and future growth. Long standing radiographs demonstrate that no shift of MA axis was observed.
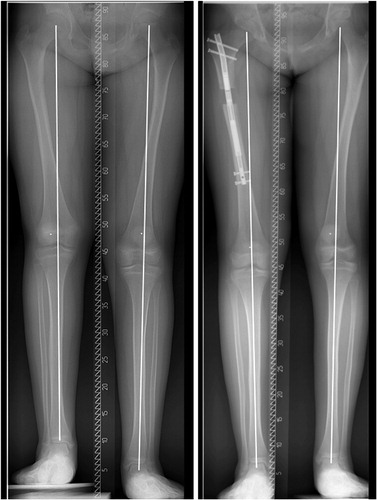
Figure 3 30-year-old man with 35 mm of tibial shortening due to traumatic injury to the proximal tibial growth plate in childhood. Furthermore, the patient had a symptomatic high-riding fibular head (a). Initial PPTA was slightly below normal (b). The patient was lengthened with a tibia Precice® nail. The fibula was osteomized, but transfixation was done only between the tibia and fibula distally to the osteotomy. This resulted in some lengthening of the fibula as well as an intended distalization of the fibular head (c). However, PPTA increased slightly from preoperatively, which was not intended (d). Delayed healing of the regenerate anteriorly (d). However, there was solid callus on 3 cortices (c, d).
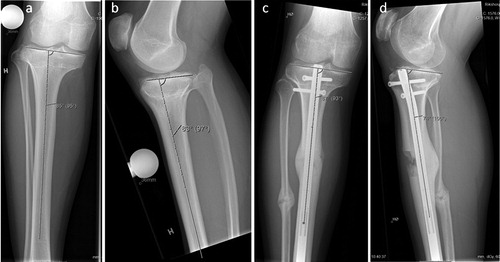
Figure 4 A 12-year-old girl with achondroplasia. She underwent consecutive 50 mm lengthenings of both femurs with the shortest available Precice nail (16.5 cm). Radiographs preoperatively (a), when lengthening was completed (b) and after consolidation (c). The nail has only one locking option proximally and distally to allow for 50 mm lengthening, despite the shortness of the nail. The patient’s femurs had not been lengthened earlier. Lengthening indices for both femurs were 0.6 months/cm, the fastest healing of all procedures included in the current study.
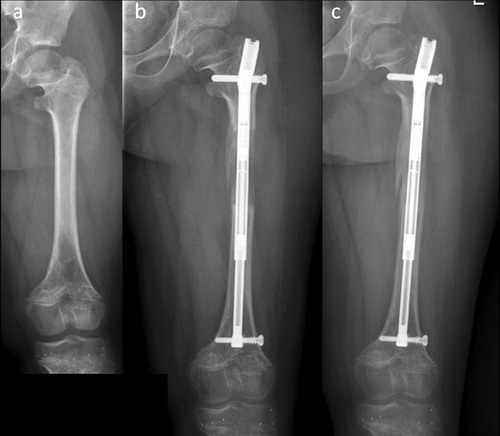
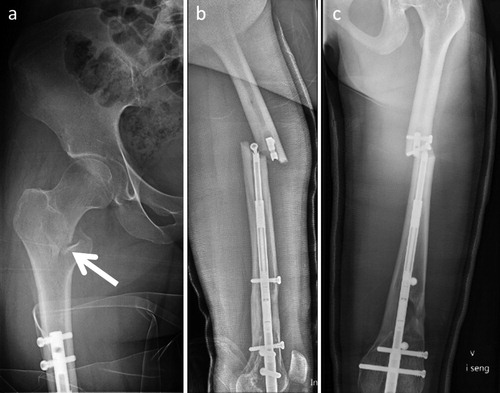
Figure 5 A 24-year-old woman who was lengthened 30 mm for idiopathic LLD with a retrograde lengthening nail. After consolidation of the regenerate she fell from a bicycle, sustaining a pertrochanteric femoral fracture (a). A 16-year-old girl with CFD, who underwent 40 mm of lengthening and correction of a valgus deformity with a retrograde lengthening nail. After consolidation of the regenerate she fell 2 m in a waterfall, sustaining a femoral fracture and breakage of the nail at the level of a locking bolt (b).