Figures & data
Table 1. Association between types of osteotomy and various clinical and preoperative radiographic variables
Figure 1. A. Preoperative radiograph of a boy, aged 7.0 years and GMFCS level V, with severe subluxation of his right hip (MP 67%). B. 1 day after femoral osteotomy (varus, derotation and shortening), pelvic osteotomy, and bilateral soft tissue releases, showing good femoral head coverage bilaterally. The cortical bone segment removed from femur has been used as autograft in the open wedge of the pelvic osteotomy. C. 7.4 years postoperatively, at an age of 14.4 years, showing satisfactory femoral head coverage bilaterally, MP 19% (right hip) and 0% (left hip)
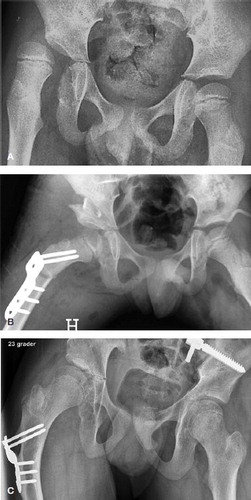
Figure 2. A. Preoperative radiograph of a girl, aged 8.1 years and GMFCS level V, with severe subluxation of her left hip (MP 74%). B. 6 weeks after femoral and pelvic osteotomies of the left hip and bilateral soft tissue releases, showing good femoral head coverage. C. 2.9 years postoperatively (age 11.0 years), showing relapse of subluxation of her left hip (MP 51%).
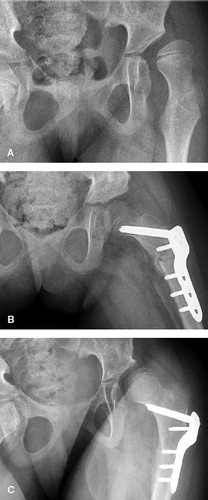
Table 2. Potential prognostic factors for poor radiographic outcome in 31 patients, estimated as relative risks (RR) for failure, using univariable Poisson loglinear regression
Table 3. Multivariable analysis of odds ratios for poor outcome, including variables with a p-value < 0.2 in univariable analysis, using multivariable exact logistic regression
Table 4. Migration percentage pre- and postoperatively (mean values with 95% confidence intervals (CI) in parentheses) of all 39 hips and comparison between hips with good and poor radiographic outcome
Figure 3. A. Preoperative radiograph of a girl, aged 5.7 years and GMFCS level V, with complete dislocation of her right hip (MP 100%) and subluxation of her left hip (MP 51%). B. 14 months after femoral and pelvic osteotomies of the right hip and bilateral soft tissue releases, showing slight subluxation of both hips (MP right hip 36% and left hip 37%). C. 7.3 years postoperatively (age 13.0 years), showing good position of right hip and deterioration of left hip (MP 64%).
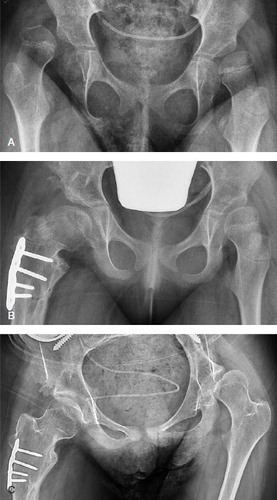
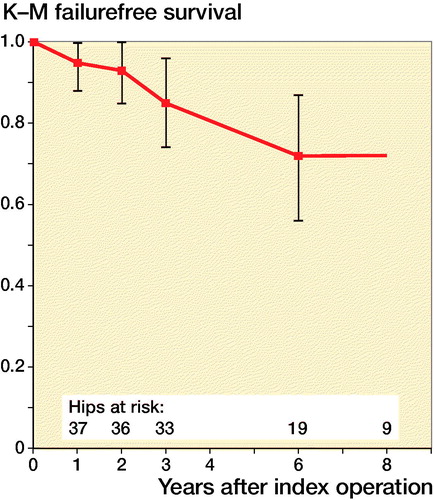
Figure 4. Kaplan–Meier survival plot (% survival with 95% confidence intervals) in all 39 hips, with time to failure (reoperation or MP ≥ 50%) as “survival”.