Figures & data
Figure 1. The manifestations and pathophysiology of chronic urticaria.
Both IgE-mediated type I and IgG-mediated type II allergies are the main pathophysiological mechanisms of CU, through which the MCs are activated and then release various inflammatory factors. Eosinophils, T cells and basophils can be recruited from the blood to the skin in response to these factors. Lower PH, higher permeability, elevated level of inflammation and the barrier disruption can be discovered in the intestine of CU patients, whose skins show wheals and angioedema.
CU, chronic urticaria; MCs, mast cells; PDG2, prostaglandin D2; TNF-ɑ, tumor necrosis factor-ɑ; IL, interleukin; FcεRI, high-affinity IgE receptor (By Figdraw).
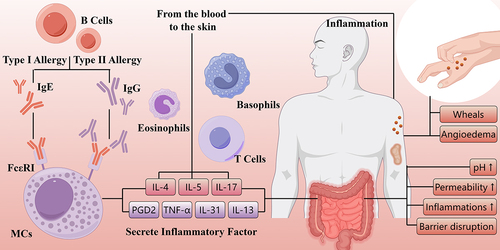
Table 1. A summary of current evidence on the association between gut microbiome composition and chronic urticaria (mainly CSU).
Figure 2. The alteration and influence of gut microbiome in chronic urticaria.
(a) Gut dysbiosis: decreased levels of SCFAs-producing pathogens, increased levels of opportunistic pathogens and relevant intestinal infections, including HP and parasite. (b) Changes of metabolites: the levels of SCFAs and unsaturated fatty acids are reduced in the intestine of CU patients, while those of LPS and purine metabolites are elevated. (c) Intensified inflammation in intestine: The upregulation of LPS and downregulation of SCFAs appear as a result of gut dysbiosis, contributing to the abnormal differentiation of naïve T cells. The levels of IL-4 and IL-17 are elevated due to more Th2 and Th17, and less Treg and Th1. MCs are activated to release some inflammatory mediators like IL-3, TNF-ɑ and histamine. (d) Roles of parasite infection: enhancing the sensitivity of MCs; breaking the mucosal barrier and amplify the intestinal permeability; producing metabolites and interact with DCs to influence the differentiation of naïve T cell; forming CIC (IgG and parasite antigen) and activate the complement system to promote the release of inflammatory mediators.
SCFAs, short chain fatty acids; HP, helicobacter pylori; CU, chronic urticaria; LPS, lipopolysaccharides; IL, interleukin; TNF-ɑ, tumor necrosis factor-ɑ; Th, T helper cells; Treg, regulatory T cells; MCs, mast cells; C3a, complement 3a; C5a, complement 5a; DCs, dendrite cells; CIC, immune complexes (By Figdraw).
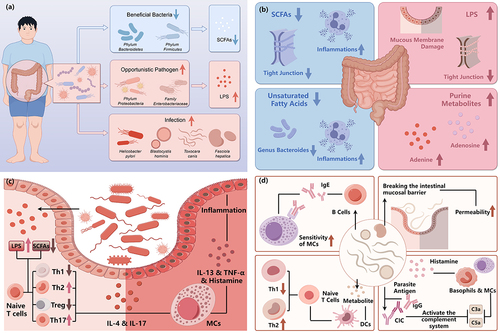
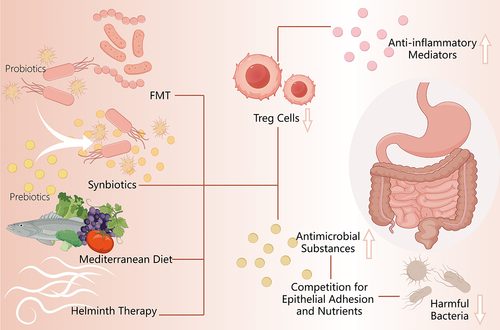
Figure 3. Summary of relevant therapies of chronic urticaria targeted at gut microbiome.
Therapeutic approaches targeting gut microbiome in chronic urticaria. Gut microbiome-based therapeutics for CU including probiotics, prebiotics, synbiotics, fecal microbiota transplantation (FMT), and others (helminth therapy and Mediterranean Diet). Treg, regulatory T cells (By Figdraw).