
Figures & data
Table 1. A consort of 33 patients who were excluded from this study, thus receiving treatment accordingly to their injury pattern. These patients did not present foveal injury on the arthroscopic evaluation (hook test – negative).
Table 2. Demographic data of the included patients.
Figure 1. (a) Intra-operative picture of the preoperative drawing, the guide-wire placement, and the 3.2 mm cannulated drill. NOTE: striped lines are depicting the patient’s ulna, while the tipped, bold line is the guide for the free-hand guide-wire placement. (b) Intra-articular guide-wire placement.
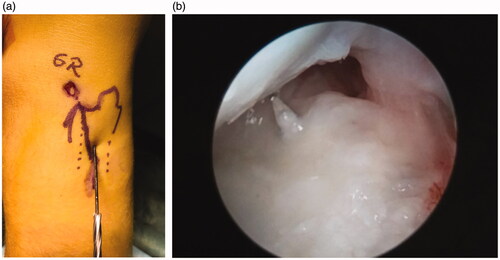
Figure 2. (a) The placement of the Micro SutureLasso Straight through the ulnar tunnel and the grasper through the 6 R arthroscopic portal. (b) The grasper is pulling the wire-loop from the SutureLasso.
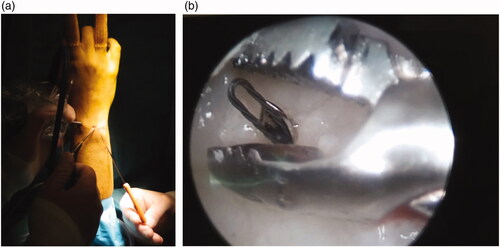
Figure 3. (a) The placement of two transosseous FiberWire sutures through the foveal aspect of the TFCC complex. The wire-loop is pulled out of the joint, through a 6 R arthroscopic portal using a grasper. (b) Then, the wire-loop is fed by the suture to be retracted back throughout the working tunnel.
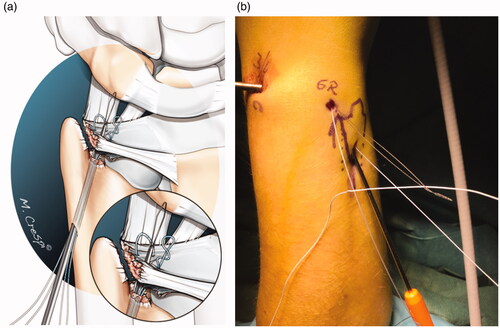
Figure 4. (a) Final fixation into the 2.5-mm predrilled bony canals in the ulna. Knotless fixation of the foveal TFCC reconstruction using 2.5 mm × 8 mm. Mini PushLock PEEK Suture Anchors using a hammer. Note: During this procedure, the tension on the arthroscopy traction tower must be lowered. (b) The final, knotless fixation of the fovea only TFCC injury.
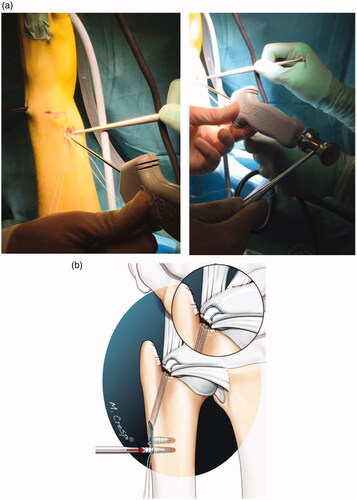
Table 3. Clinical and functional results for pain, grip strength, patient-reported functional outcome and range of motion, preoperatively and after the last follow-up.