Figures & data
Table 1. Patient demographics, smoking, and vaping history
Table 2. Clinical characteristics of vaping cases
Figure 1. Chest X ray. Chest radiographs depicting a spectrum of EVALI. (a) and (b) Chest radiographs of case 1. (a) (Day 1 of admission, pre-treatment), revealed bi-basilar haziness whereas (b) (steroid day 2), demonstrated mild improvement of left lower lobe infiltrates. (c–e) Chest radiographs of case 2. (c, d) (Day 1 of admission, pre-treatment), revealed minimal infiltrates bilaterally. Punctate density of the left upper chest is suggestive of a calcified granuloma (c), with lateral view (d) showing minimal infiltrate. (e) (steroid day 3), demonstrates clinical improvement in bilateral infiltrates. (f) Chest radiograph of case 3. (f) (Day 1 of admission, pre-treatment), revealed patchy infiltrates bilaterally
Figure 2. CT scans: computerized tomography of chest, showing a spectrum of EVALI in axial and coronal views. (a, b) Chest CT images of case 1 on admission, pre-treatment. (a) revealed bilateral ground glass opacities and interstitial infiltrates. (b) revealed prominent right hilar lymph nodes and an enlarged intrathoracic node. (c–f) Chest CT images of case 2. (c, d) (on admission, pre-treatment) demonstrating bilateral ground glass infiltrates. (e, f) (steroid day 4) showing significant improvement of lung infiltrates bilaterally. (g, h) Chest CT images of case 3 on admission, pre-treatment. (g) demonstrating diffuse patchy ground-glass opacities bilaterally. (h) showing mediastinal lymphadenopathy and interstitial infiltrates bilaterally. (i, j) Chest CT images of an asymptomatic patient with vaping history. CT images showed mild diffuse ground-glass opacities bilaterally
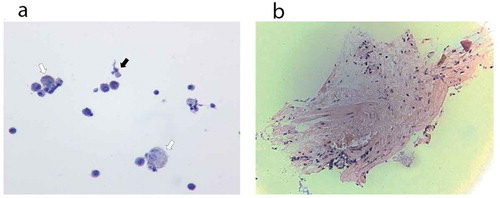
Figure 3. Histopathology. (a) Cytology from bronchoalveolar lavage fluid of case 1. The hollow arrows point to few non-vacuolated foamy macrophages, without droplet deposition. The black arrow points to one bronchial cell. (b) Pathology from lung biopsy of case 1. Minimal tissue. There is no alveolar damage observed