Figures & data
Table 1. Distribution of the studied cases according to final diagnosis of histopathology
Table 2. Distribution of to the Non-Mass findings in correlation with histopathology
Table 3. Distribution of the studied cases according to FFDM BIRADS category (n = 180)
Table 4. Distribution of Tomosynthesis findings and BIRADS categories
Table 5. Change in individual breast lesion grading on account of digital breast tomosynthesis (DBT) compared to digital mammography (DM)
Table 6. Significance of category changes after revising DBT according to lesion type
Table 7. The diagnostic performance of full-field digital mammography, Digital Breast Tomosynthesis, and combined tomosynthesis and mammography for confident breast cancer diagnosis considered histopathology as the reference standard
Figure 1. Comparison of the ROC areas of FFDM, DBT and combined FFDM and DBT for breast cancer diagnosis evidenced by histopathology as the reference standard
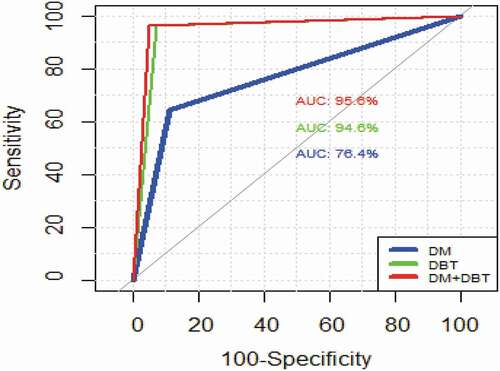
Figure 2. 49 years old case, with positive family history of breast cancer, presented for screening mammography (a) Craniocaudal and (b) Medio lateral oblique DM images of both breasts revealed suspected distortion noted at the inner portion of the left breast. (c) and (d) Craniocaudal and mediolateral oblique Tomosynthesis revealed an area of suspicious architectural distortion.(e) Ultrasound revealed an ill-defined hypo-echoic mass lesion with posterior shadowing. US guided core biopsy was performed and revealed infiltrating ductal carcinoma
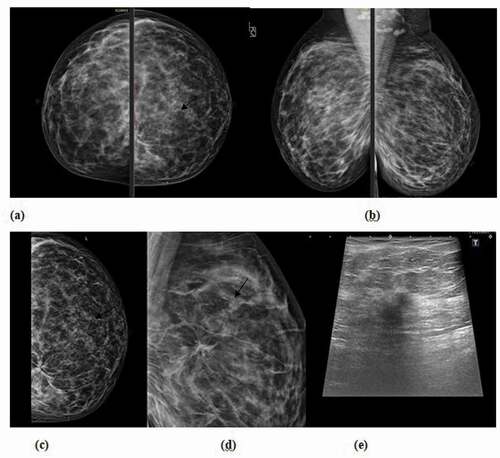
Figure 3. 54 years old patient complaining of left breast lump. (a) Craniocaudal, (b) mediolateral oblique DM images of both breasts revealed an area of focal asymmetry at the left upper inner quadrant, (c) Thin cuts tomosynthesis revealed internal fat density areas with central lucency. (d) Ultrasound showed a small hyper echoic area confined to the pre mammary region, with central cystic changes which was proved to be focal traumatic fat necrosis
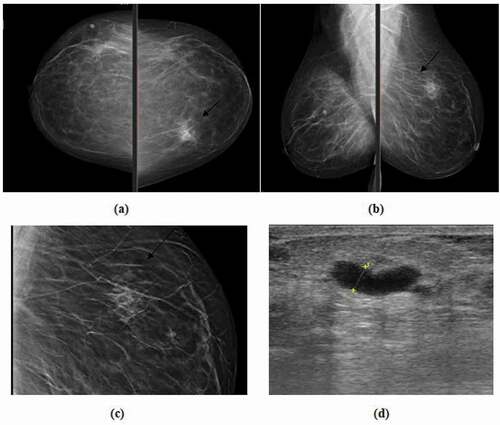
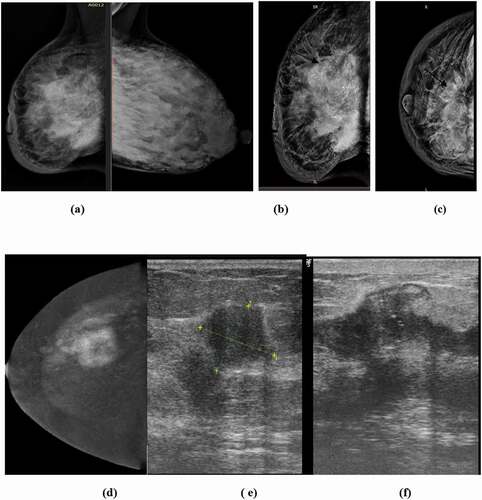
Figure 4. 32 years old lactating patient complaining of fever and right sided inflammation of the breast; (a) Medio-lateral oblique DM images of both breasts revealed right sided diffuse skin and trabecular thickening with suspicious pleomorphic segmental calcifications, (b &c) Cranio-caudal and medio-lateral oblique DBT images of right breast revealed ill-defined sizable heterogeneous mass lesion with focal retraction (tenting) of the posterior retro mammary fat and suspicious segmental calcifications, (d) CESM reveals a heterogeneously enhancing ill-defined mass lesion with related non-mass enhancement surrounding the index lesion, (e&f) Ultrasound revealed multiple ill-defined hypo-echoic masses with overlying calcifications with intervening suspicious dilated ducts. US core biopsy revealed multifocal infiltrating ductal carcinoma