Figures & data
Table 1. Reports of iliac artery dissection dissection associated with fibromuscular dysplasia.
Figure 1. (A) A 2.5-cm longitudinal intimal tear (red arrow) was found in the right common iliac artery (RCI). (B) The thrombosed false lumen involved the abdominal aorta (AA) proximally and the left common iliac artery (LCI), forming a bulging appearance. (C) The 0.7-cm adventitial rupture of the abdominal aortic (AA) dissection (red arrow), 2.5 cm above the aortic bifurcation. The probes indicate communication between the adventitial rupture of the abdominal aorta (AA), dissection of the left common iliac artery (LCI) and the intimal tear of the right common iliac artery (RCI). (D) The luminal view, with the probes showing the communication.
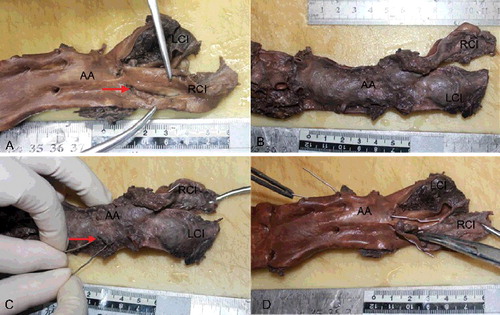
Figure 2. (A) The intact part of the aortic wall showed no histopathological change except slight intimal thickening (Masson trichrome×5). (B) Dissecting aneurysm of the abdominal aorta with longitudinal splitting of the vascular wall, ruptured adventitial layer and mural thrombus (black arrow) (HE×4). (C) Dissecting aneurysm of the abdominal aorta with longitudinal splitting of the vascular wall and splitting of elastic fibres (EvG×4). (D) Higher-power view of dissecting aneurysm of the abdominal aorta with evident thickened intima (black arrow) (EvG×10).
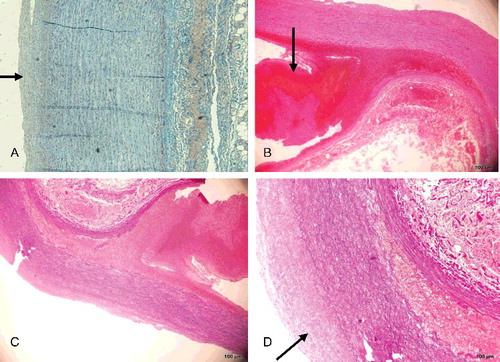
Figure 3. (A, D) Area of intimal layer rupture in the right common iliac artery (black arrow) showing hyperplasia of the intimal layer and depletion of smooth muscle cells, which are replaced with maloriented fibrous tissue (HE×4). (B, E) Area of intimal layer rupture in the right common iliac artery showing hyperplasia of the intimal layer, discontinuity of the internal elastic lamina, only scant rarefaction and fragmentation of elastic fibres and depletion of smooth muscle cells, which are replaced with maloriented elastic fibres and fibrous tissue (EvG×4). (C, F) Higher-power view of the right common iliac artery seen in (B, E) better illustrating the fibromuscular proliferation (red arrow), with rarefaction and fragmentation of elastic fibres (black arrow) in the muscularis and thinned areas of the vessel wall (EvG×10).
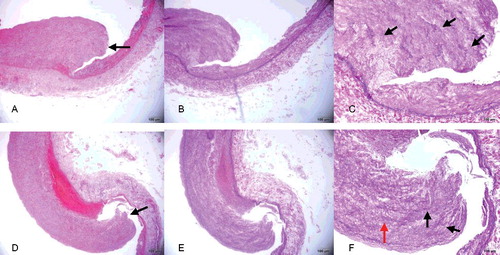
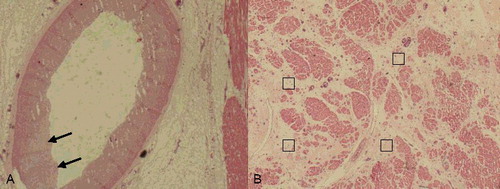
Figure 4. (A) Renal artery vessel alterations were seen in the media in areas with thick intima and fibroplasia with disorganization of smooth muscle cells (black arrow) (HE×4). (B) In the renal arteries, alterations in the media were seen in areas with thick intima (red arrows), fibroplasia with disorganization of smooth muscle cells and loss of elastica in the muscularis (black arrows) (EvG×4). (C) Higher-power view of the renal artery showing fibroplasia with disorganization of smooth muscle cells and loss of elastica in the muscularis (black arrow) (EvG×10).
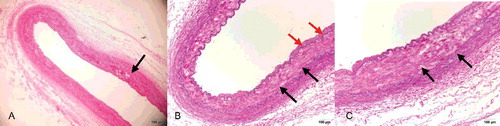
Figure 5. (A) The left anterior descending artery showed slight intimal thickening and internal elastic lamina discontinuity (black arrows) (HE×2). (B) Interstitial fibrosis (□) with capillary proliferation of left ventricle (HE×2).