Figures & data
Figure 1. The role of omental adipocytes in tumour development and metastasis.
In omental adipocytes exposed to asbestos, MCP-1 secretion is increased and adiponectin secretion is reduced, resulting in an inflammatory reaction and mesothelial cell hyperplasia that induces the development of mesothelioma. Among adipokines from omental adipocytes, leptin, adiponectin, IL-8, IL-6, and MCP-1 induce tumour cell homing, survival, proliferation, migration, invasion, and chemo-resistance in metastatic tumour cells in the omentum. VEGF, VEGFR3, and CD106 enhance angiogenesis. Metastatic tumour cells in the omentum promote lipolysis, and the generated fatty acids are transferred to tumour cells and used in β-oxidation. Oleic acid activates the PI3K/AKT pathway and promotes cancer cell invasiveness. PUFAs activate PPARβ/δ in macrophages and polarizes them into tumour-associated macrophages. MCP-1, monocyte chemoattractant protein 1; IL, interleukin; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor; PUFA, polyunsaturated fatty acid.
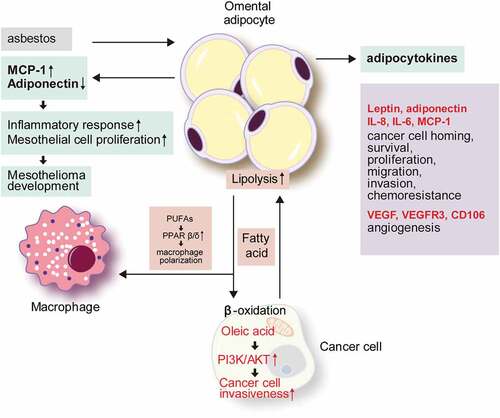
Figure 2. The role of bone marrow adipocytes in solid tumour metastasis and hematologic tumour development.
Bone marrow adipocytes are involved in solid tumour metastasis via the secretion of various adipokines. Leptin enhances cancer cell colonization and adipogenesis, which induces tumour progression. Adiponectin promotes tumour growth and migration. IL-6 increases tumour cell survival. The CXCL1/CXCL2 axis increases osteoclastogenesis, and suppresses the anti-tumour immune response. The COX-2/PGE2 axis represses the immune response, and induces tumour-related bone degradation. Adipocytokines are also involved in hematologic tumour development and progression. Leptin suppresses apoptosis and activates autophagy, which induces chemo-resistance. Reduction of adiponectin secretion promotes the progression of MGUS to myeloma. Adipsin and CXCL12 participate in drug resistance. IL-6 and visfatin are involved in myeloma cell progression. Tumour cells of solid tumours and hematologic tumours receive fatty acids transferred from the adipocytes. In solid tumours, AA activates the PI3K/AKT and NF-κB pathways that induce cancer cell proliferation and invasion. AA also activates COX-2 and PGE2 that repress the immune response and induce tumour-related bone degradation. In hematologic tumours, linoleic acid and oleic acid increase the proliferation of myeloma cells. CXCL, (C–X–C motif) ligand; COX-2, cyclooxygenase-2; PGE2, prostaglandin E2; MGUS, monoclonal gammopathy of undetermined significance; IL, interleukin; PI3K/AKT, phosphoinositide 3-kinase/protein kinase B; NF-κB, nuclear factor-kappa B.
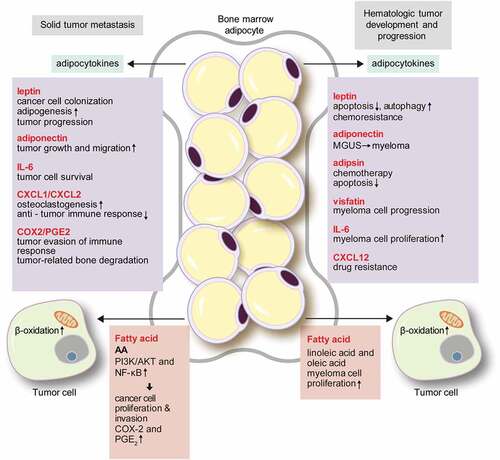
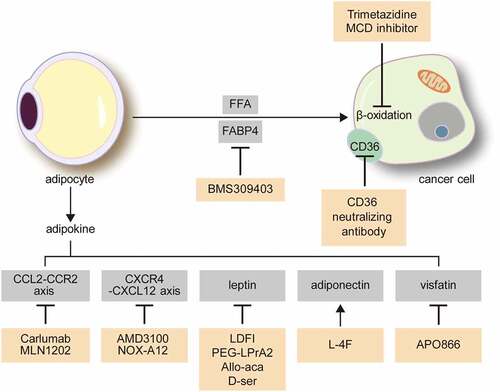
Figure 3. Possible treatment targets for the interaction between cancer cells and adipocytes in the omentum and bone marrow.
CCL2/CCR2 axis inhibitors are modulators of adipokines. Calruman and MLN1202 are monoclonal antibodies against CCL2 and CCR2, respectively. CXCR4/CXCL12 axis inhibitors include AMD3100 and NOX-A12, which are inhibitors for CXCR4 and CXCL12, respectively. L-4F, an apolipoprotein mimetic, increases the adiponectin level and has an anti-tumour effect. APO866 is a visfatin inhibitor. Lipid metabolic interactions between tumour cells and adipocytes are potential therapeutic targets. Trimetazidine and malonyl-CoA decarboxylase (MCD) inhibitors are inhibitors of fatty acid β-oxidation in tumour cells. BMS 309403 inhibits FABP4, a fatty acid transporter, and CD36 blocking antibody blocks CD36, a transmembrane protein for fatty acid uptake. CCL2, C-C motif chemokine ligand 2; CCR2, C-C motif chemokine receptor 2; CXCL, (C–X–C motif) ligand; CXCR, (C–X–C motif) receptor; FABP4, fatty acid binding protein 4.