
Figures & data
Figure 1. Rationale and design of procedures.
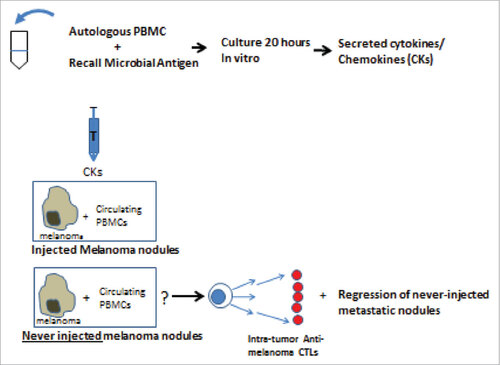
Figure 2. Photographs of patients with cutaneous/subcutaneous metastases experiencing regressions after intralesional CKs. A. 70 year old female: large subcutaneous metastases undergoing rapid rejections. Only checked nodules injected. Dotted nodules are regressing. Collapsing lesion 12 was never injected. Some nodules marked for excision. B. 50 year old female: in transit metastases of left leg and inguinal scar, 4 positive lymph nodes, and no response to chemotherapy. Only circled area injected. Complete regressions and survived disease free for >5 years. Lost to follow up. C. 62 year old male: 6 lesions increased to 57+ small metastases on head and neck. Only lesions on right side injected. All lesions regressed: a 2 × 3 cm mass developed in neck and spontaneously regressed. Needle biopsy showed only residual pigment in melanophages. Became NED after 2 years; died of other causes at age 86, 24 years after entering the study. D. 55 year old male entered with disseminated subcutaneous metastases, face, chest, arms and leg; stage IV-M1a. All lesions including never-injected nodules on arm regressed by 6 months after entry.
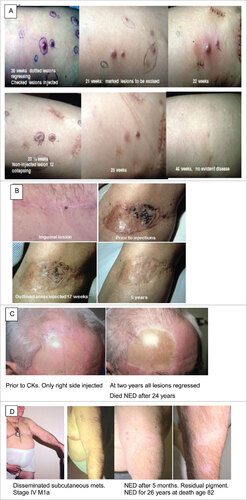
Table 1. Concentrations of selected CKs prepared from normal individuals and from and injected into patients who experienced CRs.
Figure 3. Ex-vivo measurements of (TIL) or blood lymphocytes (BL) to kill autologous melanoma cells. Cytotoxicity presented at increasing effector to melanoma target cell ratios. Each figure is representative of 6 to 10 experiments (A) Comparing the same number of lymphocytes, TIL are more lytic than BL. TIL•, BL ▪. (B) TIL preferentially kill autologous melanoma cells as compared to allogeneic cells, consistent with MHC restriction. Pt C TIL•, Pt M TIL▪ (C) Killing is MHC restricted and not due to NK cells. Pt C BL •, Pt C BL minus NK ▪, Pt F BL ▴, Pt F BL minus NK ▾, (D) Depletion of CD8 T cells abrogates the killing. BL •, BL minus CD8 T▪ (E) Repeated injection in 3 patients of CKs mixed with irradiated autologous melanoma cells over many weeks increases the killing ex-vivo.
Figure 4. Chart of numbers of patients with regressing and recurrent metastases.
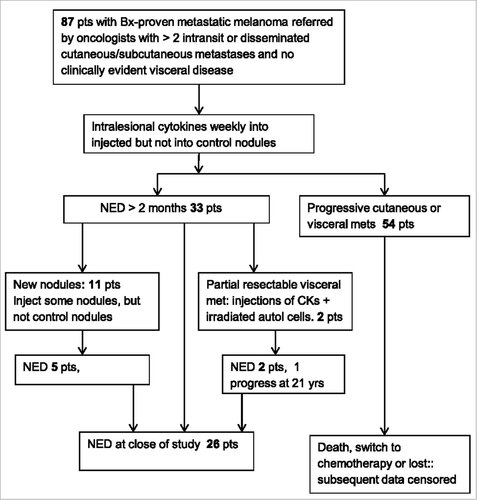
Table 2. Clinical Outcomes: Summary of responses and survival. NED = No Evident Disease by examination and chest x- ray for at least 8 weeks followed by negative scans. The table provides median and range of data on all 87 patients for: time to NED, the % of patients achieving NED for greater than 2 months, and the % of patients with a cumulative duration of NED of 2, 3 and 5 years. The table also presents median and range of overall and disease-free survival from entry at different times. Because some patients relapsed after being free of disease for protracted periods, the % of subjects surviving free of disease for 1 to 5 years after entry is less than the cumulative duration of disease free periods. Also a few disease-free patients were lost to follow up.
Figure 5. Melanoma status of all patients ranked by the duration of follow up in months and years after entering. The time line for each patient is censored at death, initiation of chemotherapy, or when last examined. Red indicates no clinically evident disease (NED) by examination and chest x-ray for at least 8 weeks, and subsequent negative scans. Several patients had NED# when lost to follow up. Black indicates presence of metastatic melanoma. Note, many patients had prolonged periods of stable or slowly progressive disease. 4 patients who had NED for >2 years experienced a late relapse as indicated. A Patient was experiencing a rapid regression of many metastases after 27 weeks of CK injections (with dense lymphocytic infiltrates in never injected nodules) when she switched to a geographically closer physician, and began receiving injections of an allogeneic melanoma vaccine to enhance immune responses. Within 8 weeks after the last CKs and after 4 weekly injections of vaccine she demonstrated NED. Subsequent indicated recurrences were treated by irradiation or excision.Citation61 B The recurrence of melanoma after 20 years of NED subsequently responded to Ipilimumab.
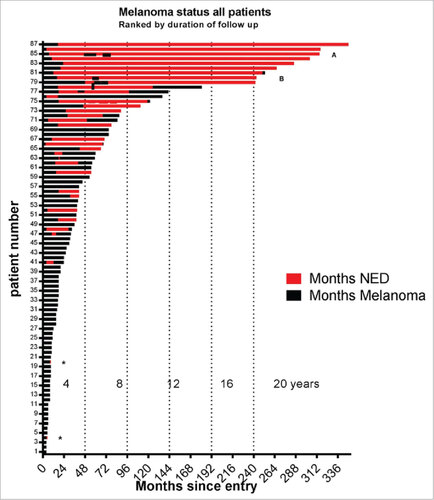
Figure 6. A Kaplan-Meier plot of overall survival on study and after switching to chemotherapy. Tick marks indicate alive at end of study or when lost to follow-up.
Table 3. Clinical stages of patients at entry and frequency of CRs. All patients had developed 2 to over 100 palpable cutaneous and subcutaneous metastases during the previous 2 months, and most continued to have new nodules during the first few weeks on study. 30 patients had failed prior chemotherapy ending 2+ months before entry.