
Figures & data
Table 1. RCC antigens recognized by spontaeously arising tumor-reactive CD8 CTL clones
Figure 1. RCC has a high objective response rate to immune checkpoint blockade despite low TMB. Median number of coding somatic mutations per megabase (MB) of DNA for 27 tumor types is plotted in log scale versus objective response rates for patients who received PD-1 or PD-L1 inhibitors as described in published studies. RCC is within the top 25% of objective response rates while being within the bottom 33% of median number of coding somatic mutations per MB. MMRd denotes mismatch repair-deficient, MMRp mismatch repair proficient, and NSCLC non-small cell lung cancer. Reproduced from Yarchoan, Hopkins & JaffeeCitation55 with copyright permission
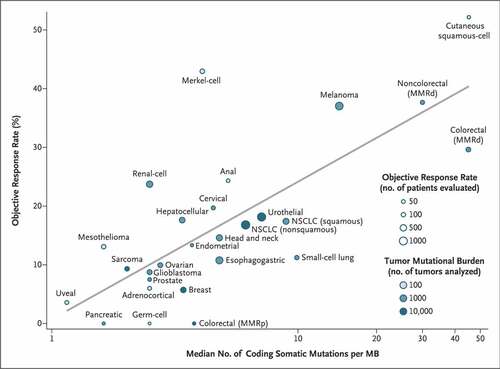
Table 2. Clinical testing of single antigen-specific vaccination or T-cell engaging therapy for advanced RCC
Table 3. Clinical testing of multiple antigen vaccines for advanced RCC
Table 4. Active trials with engineered T-cell therapy enrolling metastatic RCC patients