Figures & data
Figure 1. Ex vivo biopsy simulation method with standard needle and Forsvall needle prototypes. (A) Schematic depiction of standard Tru-Cut biopsy needle mechanism. (B) Schematic depiction of Forsvall needle biopsy mechanism. (C) The five needles used in the ex vivo simulation were a standard 18 G Tru-Cut needle (Bard) and four versions of the Forsvall 18 G stainless steel needle prototype: Facetted tip with no coating, facetted tip with gold + PEG coating, pencil point tip with no coating, and pencil point tip with gold + PEG coating. Note that the opening of the Tru-Cut needle is in the direction of travel, the opening of the Forsvall needle is in a 90-degree angle to the direction of travel. In the ex-vivo simulation the needles were used in this same order until all punctures were completed. (D) Schematic depiction of the experimental workflow. First, fresh colons were obtained after colon cancer surgery and opened to form a 5 × 8cm rectangle. This rectangular piece of colon was then mounted on a special bracket with the mucosal side up. A randomization pallet consisting of 50 evenly spaced holes labelled A–E and 1–10 was mounted over the colon. A card was drawn from a randomization deck of playing cards with labels corresponding to the holes on the randomization pallet. The corresponding hole was then punctured with the next needle in the series. The needle was immediately submerged in a tube filled with culture media to a depth of 6 cm, opened and closed to dislodge any collected material, and then removed. The culture media was plated on a code-labelled blood agar plate and incubated overnight, and the number of colonies was counted blindly to avoid bias. (E) Photograph of a colon mounted on the bracket with the randomization pallet placed on top, as viewed from above.
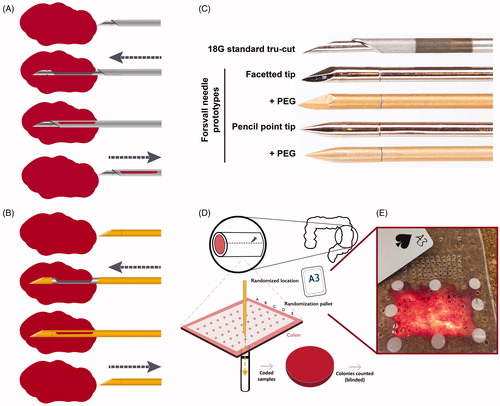
Table 1. Baseline characteristics of patients and colon specimens.
Figure 2. Effect of physical properties and needle coating on bacterial translocation in a pilot experiment. (A) Representative images of a standard Tru-Cut biopsy needle (Mermaid 18 G) after a puncture through a simulated colon. Left images show the gap between the inner and outer needle in a closed (top) and opened (bottom) state. Right image shows the rough, highly echogenic area, used for enhancing ultrasound reflection and visualization of the needle within the body in other types of biopsy. The highly echogenic area has no use in TRbx because a needle guide is used to locate the needle tip. Arrows indicate areas of visible faecal matter and tissue collection. (B) Gold + PEG coated rod prototype needle after puncture of a piece of meat covered in faecal matter, simulating the rectal wall. No foreign matter was visible at this magnification. (C) Number of bacterial colonies translocated when a piece of meat covered in faecal matter was punctured with three different standard Tru-Cut needles and ten versions of the rod prototype needle with different combinations of surface coatings. The average bacteria translocated by all three standard needles (pooled) was set to 100% and the percentage translocated by each rod prototype needle was calculated relative to this number.
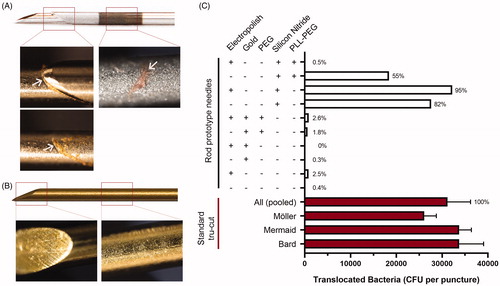
Figure 3. Standard Tru-Cut needle and prototype needle after puncture through an ex vivo human colon. (A) Representative images of the gap between the inner and outer needle parts of a standard 18 G Tru-Cut needle (Bard 18 G) when closed and partially open, following puncture of an ex-vivo human colon. White arrows indicate areas of visible fecal matter and tissue collection. Red line in the ‘open’ image indicates the position of the outer needle when closed, please note the extensive visual contamination. (B) Representative images of a 18 G Forsvall needle prototype (pencil tip with gold + PEG) following puncture with of an ex-vivo human colon, images show corresponding locations to images in A, closed and partially open. No foreign matter was visible at this magnification. (C) Mean number of colonies (CFU) translocated per puncture through each colon by the four Forsvall needle prototypes and the standard Tru-Cut needle. Percentages are indicated above each bar with the mean bacteria translocated by the standard needle set as 100% for each colon.
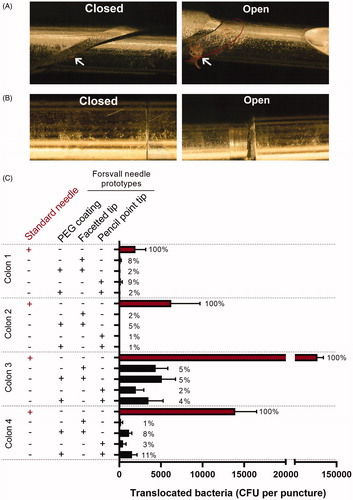
Table 2. Percent reduction of translocated bacteria for each variation of the Forsvall prototype needle, as well as the four prototype needles grouped, relative to the standard Tru-Cut needle (BARD 18 Gauge 20 cm Tru-Cut biopsy needle for MAGNUM biopsy gun).
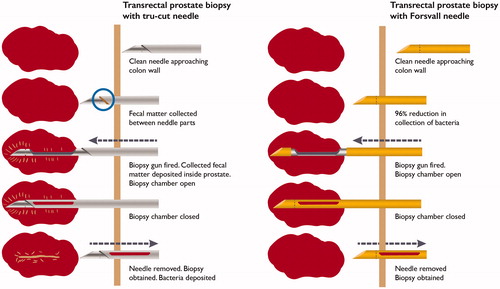
Figure 4. Schematic depiction of TRbx and bacteria/fecal matter deposition when using a standard tru cut needle (left) and the Forsvall needle prototype (right).