Figures & data
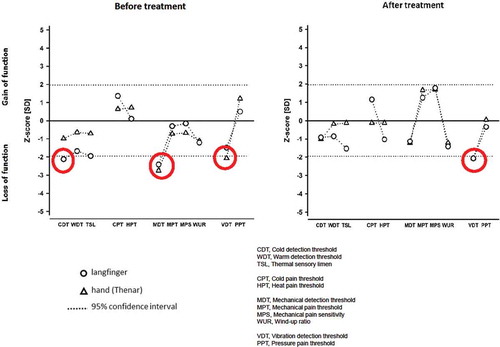
Figure 1. Angiography before and after treatment. Angiographic images showing the status of peripheral vessels in fingers. The pre-treatment picture show open arteries in the right forearm. The digital arteries in the hand are displayed extraordinary gracile. The blood-flow in the arteries are reduced, even if the fingers are stimulated with mild heat or undergoing exercise. The post-treatment images still show reduced peripheral vascularisation, however, the digital arteries are more vasodilated and less gracile compared with the pre-treatment display.
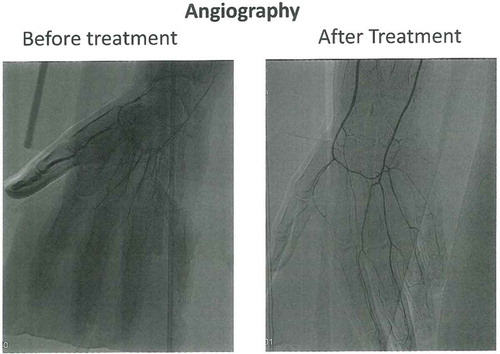
Figure 2. Thermography before and after treatment. Thermographic images of the hands taken on 3 different occasions. (A) the initial examination 05.02.2015; (B) follow up examination immediately prior to BTX-A treatment 19.05.2015 and (C) follow up examination after BTX-A treatment 17.11.2015. On the first and the third occasion, the patient’s hands was subjected to a mild cold provocation test (2-minute period of convective cooling using a desk top fan). The images were taken after the patient had had sat in the laboratory wearing warm clothes to ensure he was very mildly hyperthermic at the time of the examination. This was confirmed from the patient’s reported subjective feeling as well as from thermal facial images showing that the nose (open arterio-venous anastomoses) was vasodilated. The hand images were taken immediately after the patient arrived at the laboratory (on arrival), after the patient had been warmed up (prior cooling) and 3 minutes after the end of the cold provocation period (3 min recovery).
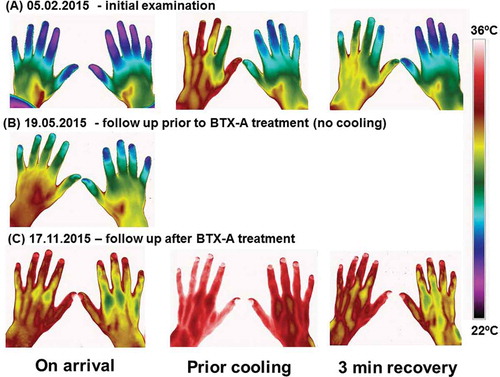
Figure 3. Quantitative Sensory Testing (QST) before and after treatment. The z-transformed pattern of 11 QST subtests (shown without dynamic mechanical allodynia (DMA) and paradoxical heat sensation (PHS), which were normal). QST reveals thermal hypoesthesia of cold stimuli (CDT) in the directly affected area (middle finger), most likely related to the loss of small fiber function (Aδ fibres). The ability to detect minimal mechanical stimuli (MDT) is reduced within (long finger), as well as outside (thenar of the same hand) the affected area, as is the ability to detect vibration (VDT) in the hand area. These mechanical deficits reflect most likely a loss of function of large diameter fibers (Aβ fibres). With the exception of VDT, treatment with BTX-A normalised the QST pattern. The red circles in the figure indicate values measured outside the two Standard Deviation (SD).