Figures & data
Figure 1. 1 A. Anteroposterior, 1B. oblique and 1 C. lateral radiographs of bilateral hands demonstrating mild degenerative carpal and interphalangeal joint changes with no other osseous or soft tissue abnormalities.

Figure 2. 2 A. T2 axial, 1B. T1 axial, 1 C. T1 coronal, and 1D. T2 coronal magnetic resonance imaging of the left wrist demonstrating abnormal enlargement with mixed signal involving the median nerve just proximal to the carpal tunnel (yellow arrow). Note the coaxial cable-like appearance on the coronal imaging and honeycombing on the axial consistent with fibrolipomatous hamartoma.
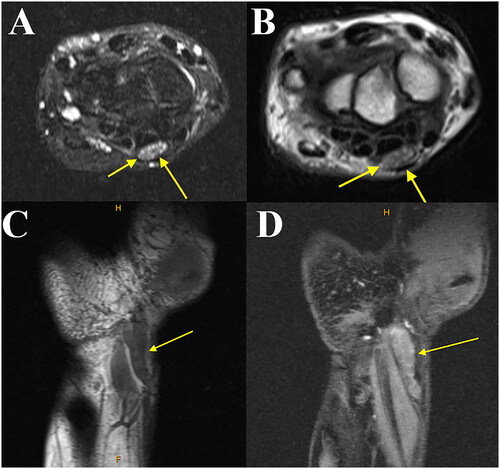
Figure 3. Intraoperative image of left wrist demonstrating a planned extensile approach (bold line) to the carpal tunnel.
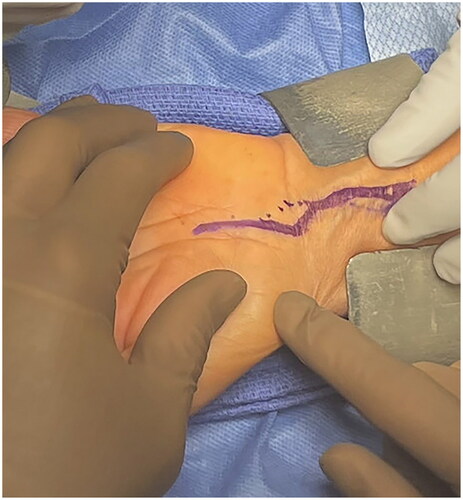
Figure 4. Intraoperative image of the left wrist. Tenosynovectomy is performed demonstrating extensive tenosynovitis (yellow arrow). The flexor tendons underlying the tenosynovium are seen in the bed of the wound (blue arrow). The retractor at the bottom of the image is protecting the median nerve from inadvertent injury.
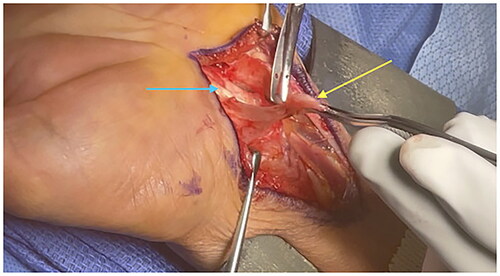
Figure 5. Intraoperative image of the left wrist. The median nerve is seen with an abnormal fusiform mass (yellow arrow). Micro-instrumentation is used to reveal the underlying mass to further assess for possible removal.
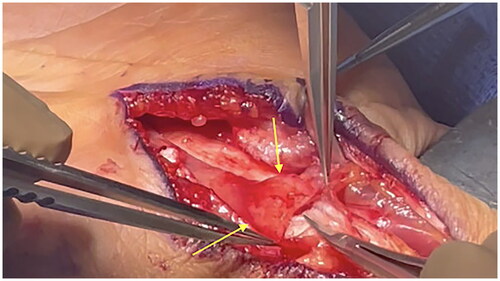
Figure 6. Intraoperative image of the left wrist. The median nerve is positioned on a background with fibrolipomatous hamartoma demonstrated next to the measuring utensil. Neurolysis of the epineurium has been performed and the mass is seen to be intimately associated with the underlying fascicles preventing excision.
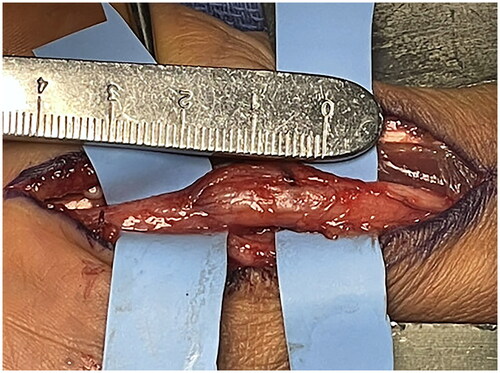
Figure 7. Intraoperative image of the left wrist. The median nerve is wrapped with a collagen nerve wrap to prevent adhesions and scarring of the nerve postoperatively.

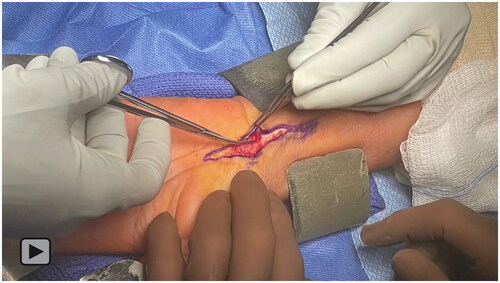
Video 1. Intraoperative video of the left wrist demonstrating an extensile approach to the carpal tunnel for decompression and collagen nerve wrapping of a fibrolipomatous hamartoma of the median nerve.