Figures & data
Figure 1. Example of vertical slight, persistent positional nystagmus evoked by symmetrical positioning during PAN I. (A) Sitting position. This position has been maintained for a longer time before the measurements therefore the vertical semicircular cupulae are already deflected upward and adapted to this situation. (B) From sitting to 30° prone (no nystagmus because the position of the vertical cupulae does not change), (C) from 30° prone to head-hanging prone (upbeat nystagmus because of the deflection of the anterior and posterior cupulae (curved arrows)), (D) from head-hanging prone to sitting (downbeat nystagmus for over 100 s), and (E) from sitting to supine: again upbeat nystagmus (because of the deflection of the anterior canal cupula).
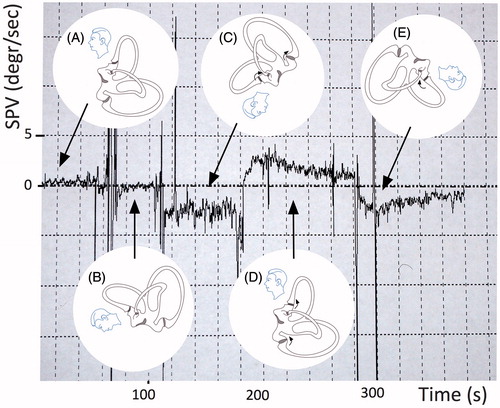
Table 1. Direction and intensity of the vertical nystagmus elicited by symmetrical positioning (around the y-axis with pitch rotation).
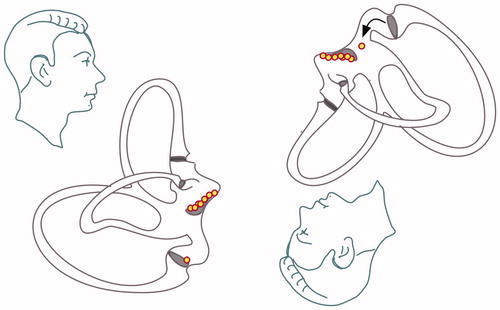
Figure 2. Horizontal short arm canalolithiasis causing unilateral crescendo–decrescendo apogeotropic horizontal nystagmus when the involved ear is lowermost.
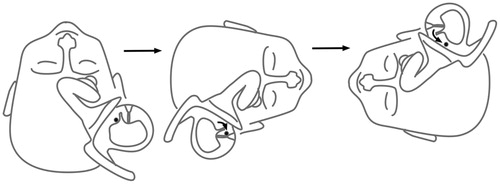
Figure 3. Horizontal light cupula.

Table 2. Possible nystagmus types in peripheral positional vertigo and dizziness – a hypothetical topodiagnostic classification based on the pathophysiology of the vestibular labyrinth (the nystagmus in posterior canalolithiasis is called upbeat-geotropic, because in the Dix–Hallpike position the patient’s head is hanging upside down and an upbeat nystagmus with a fast component toward the centre of the earth also beats towards the top of the head. On the other hand, nystagmus beating down, in the direction of the chin, such in anterior canalolithiasis, is called positional downbeat nystagmus; although in head-hanging position, this is in fact apogeotropic. The torsional component is named by the fast movement of the upper pole of the eyes).
Figure 4. New classification is suggested, based on the dynamics of the nystagmus (persistent vs. crescendo, decrescendo) and on the plane of the provoked nystagmus (vertical vs. horizontal).
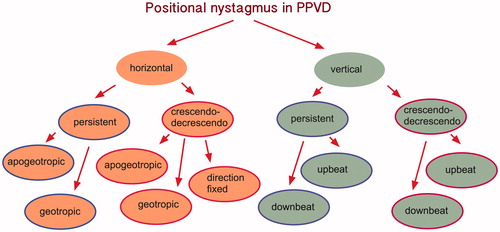
Figure 5. Posterior cupulolithiasis: in cases of posterior cupulolithiasis, depending on the precise position of the inferior ampulla, either no nystagmus or a slow downbeat nystagmus should ensue when the patient is positioned from sitting to the Dix–Hallpike position. This downbeat nystagmus of frequently seen after a successful Epley manoeuver because the debris is moving into the utriculus and is deposited in its most inferior part, which is the posterior ampulla.
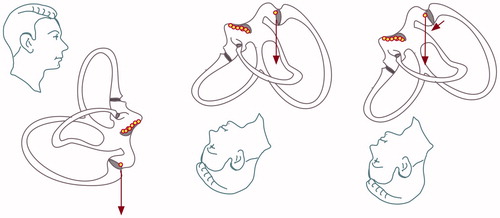
Figure 6. Vertical canal light cupulae.
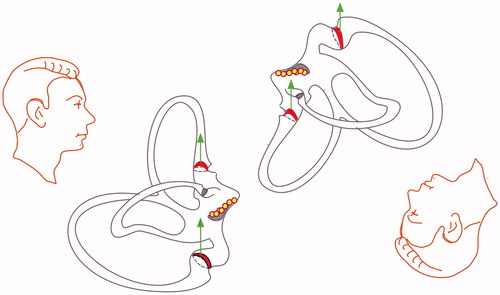
Figure 7. Posterior short arm canalolithiasis.