Figures & data
Figure 1. (A) Delayed axial technetium-99m sestamibi single photon emission computed tomography (SPECT) fused with axial CT shows focally retained activity at the inferior aspect of the right lobe of the thyroid gland, with indentation along the inferior margin of the lower pole of the right thyroid lobe. (B) Transverse colour doppler ultrasound of the right thyroid lobe demonstrates a hypoechoic extrathyroidal nodule posterior to the lower pole of the right thyroid with internal vascularity and calcifications, correlating to the abnormality on SPECT/CT.
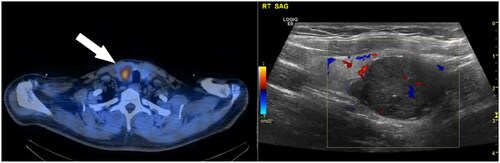
Figure 2. (A) Anterior and posterior whole-body planar images from a technetium-99m-methylene diphosphate (MDP) bone scan show increased tracer uptake secondary to hyperparathyroidism, at the left acromioclavicular joint (black asterisk), cervicothoracic junction (grey arrowhead), costochondral junctions bilaterally (black arrowhead), left iliac bone (grey arrow, biopsy-confirmed brown tumour) and right patellofemoral joint (black arrow). (B) Anteroposterior radiograph of the left shoulder showing osteolysis of the distal clavicle. (C) Axial CT of the spine showing a pathological fracture of the T1 spinous process, secondary to a brown tumour. (D) Axial CT through the chest showing an expansile lytic lesion of the anterior left 5th rib, in keeping with a brown tumour. The increased uptake on bone scan along the remaining costochondral junctions was non-specific. (E) Anteroposterior radiograph of the right knee showing a large lucent lesion in the patella, consistent with a brown tumour.
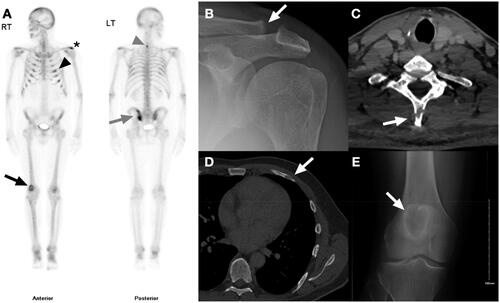
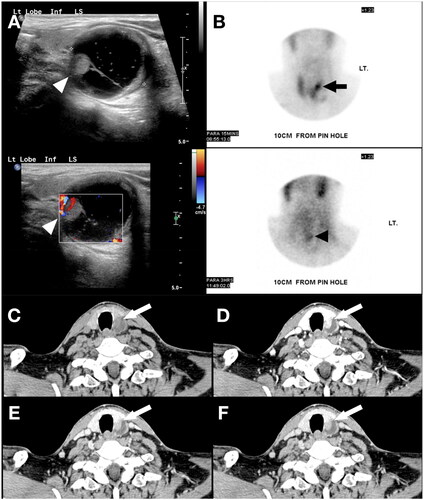
Figure 3. (A) Ultrasound of the thyroid demonstrates a 3.1 cm complex cyst centred on the left lobe of the thyroid, with a moderately thick wall, central cystic components and a hypervascular mural nodule protruding intraluminally (white arrowhead). (B) Technetium-99m sestamibi early and delayed images demonstrate focal uptake corresponding to the hypervascular nodule identified on US in the left lobe of the thyroid gland (black arrow). There is retention of radiotracer uptake on delayed images within the nodule (black arrowhead) with washout of the background thyroid activity. (C-F) Multiphasic CT images of the neck with initial non-contrast phase followed by 30, 60 and 90 second post-contrast delays, demonstrate a 3.3cm mixed solid-cystic lesion posterior to the left lobe of the thyroid gland, containing a solid nodule which demonstrates hyperenhancement and washout (white arrow), with Hounsfield Units of 36, 131, 104 and 97 respectively.