Figures & data
Figure 1. Three-dimensional pelvic coordinate system. The most ventral points were automatically located on the anterior superior iliac spine and pubic tubercles bilaterally (red points) and were used to establish the three-dimensional pelvic reference frame. The anterior pelvic plane, or coronal plane (red plane), consisted of the anterior superior iliac spine and the pubic tubercle points bilaterally. The sagittal plane (green plane) contained the line (dashed line) connecting the two midpoints of the bilateral anatomical landmarks and was normal to the APP. The axial plane (blue plane) was normal to both coronal and sagittal planes.
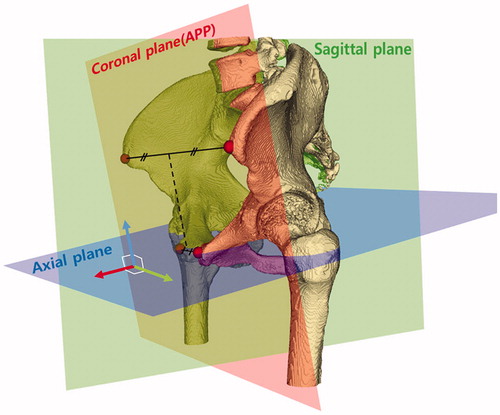
Figure 2. An algorithm for determining the acetabular rim plane, which consisted of six steps. Step 1: Specifying the ROI for each femoral head (Red box). Step 2: Identifying a best-fit sphere (blue) using planar circles (red) detected by SHT. Step 3: Reconstructing each slice using the scan line. The yellow points detected by the corner detection algorithm were candidates for the acetabular rim points. Step 4: Generating the pseudo plane and acetabular coordinate system. The blue points were selected by a RANSAC algorithm; the red points were determined as outliers. The pseudo plane (dashed line) was determined by blue points, and the plane (solid line) was obtained by moving the pseudo plane 1 cm in the direction of -ZA. Step 5: Determining the true acetabular rim points. The true rim point was defined by a virtual ray. The direction of the virtual ray was adjusted by changing the azimuth (θ) and angle (φ). The first-hit voxels were defined as the true rim points. Step 6: The plane fitting the acetabular rim points (yellow) determined the true acetabular rim plane (white).
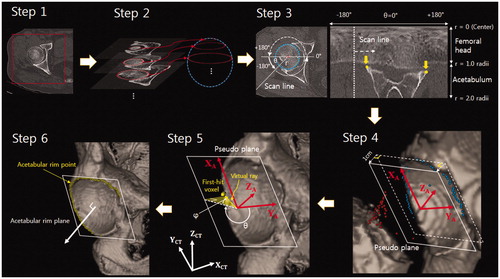
Table 1. Elapsed time of the algorithm for two phase including manual operation (n = 20).
Table 2. ICC values for calculation of the angles on two separate occasions (n = 20).
Table 3. Acetabular inclination and anteversion by age and gender (n = 200).
Figure 3. Acetabular inclination by age and sex. Regression analysis indicated no evidence of an association.
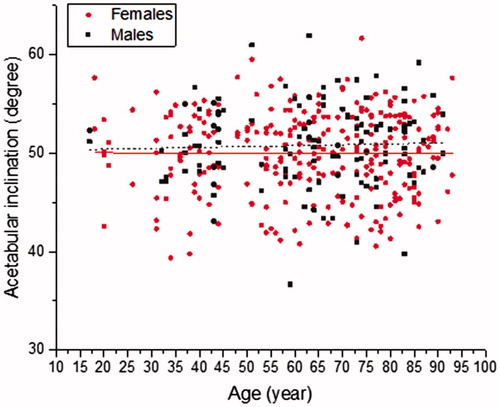
Figure 4. Acetabular anteversion by age and sex. Regression analysis indicated no evidence of an association.
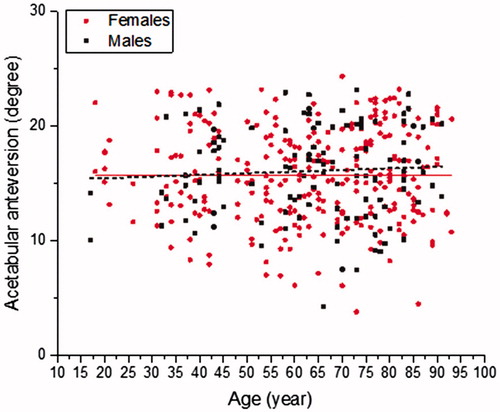
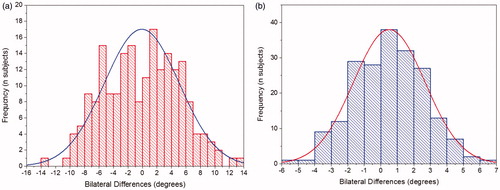
Figure 5. Frequency and magnitude of intra-patient bilateral differences (left minus right). Relative symmetry was shown for (a) anatomic anteversion and (b) anatomic inclination.