Figures & data
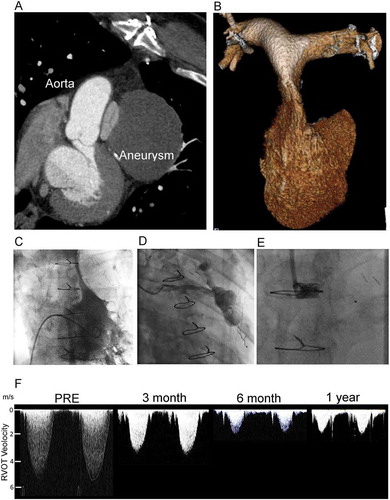
Figure 1. Acquired right ventricular outflow tract (RVOT) obstruction due to coronary graft aneurysm treated by percutaneous graft occlusion. (A) 2D multidetector computed tomography (MDCT) showing compression of the pulmonary valve between the graft aneurysm and the native aorta. (B) 3D MDCT reconstruction of the RV and pulmonary arteries showing the slit-like appearance of the main pulmonary artery. (C) Right ventriculography shows a minimum dimension of 2.2 mm, with an invasive pressure of 83 mmHg. (D) Graft angiography demonstrates the large aneurysm and feeding vessel. (E) An 8-mm AVPII device was used to occlude the graft with the expectation that thrombus would form and ultimately resorb. (F) Serial non-invasive Doppler assessments of the RVOT velocity show progressive and then stable reduction from 5.1 m/s at presentation to 1.7 m/s in follow up. RV dimensions, and hypertrophy normalize over this period. The patient was well and able to return to work at 6 months