Figures & data
This illustration is not entirely correct, as in most cases there appears to be very little or no muscle left on the bone since the tear occurs at the insertion rather than in the muscle belly. However, the figure correctly describes the most common form of trauma, affecting the right puborectalis muscle, with retraction of muscle fibers perianally, and its most common cause at the time (i.e., forceps delivery).
Reproduced with permission from Citation[2].
![Figure 1. Right-sided avulsion seen from the caudal view.This illustration is not entirely correct, as in most cases there appears to be very little or no muscle left on the bone since the tear occurs at the insertion rather than in the muscle belly. However, the figure correctly describes the most common form of trauma, affecting the right puborectalis muscle, with retraction of muscle fibers perianally, and its most common cause at the time (i.e., forceps delivery).Reproduced with permission from Citation[2].](/cms/asset/0757342e-da07-480e-af50-3eecc1947250/ierb_a_11205123_f0001_b.jpg)
The vulva, mons pubis, clitoris, perineal muscles and perineum to the anus, as well as peri- and postanal skin and and some of the fibrofatty tissue of the ischiorectal fossa have been removed to allow access to the puborectalis muscle.
Reproduced with permission from Citation[61].
![Figure 2. Intact puborectalis muscle in a fresh cadaver, dissected from caudally.The vulva, mons pubis, clitoris, perineal muscles and perineum to the anus, as well as peri- and postanal skin and and some of the fibrofatty tissue of the ischiorectal fossa have been removed to allow access to the puborectalis muscle.Reproduced with permission from Citation[61].](/cms/asset/9fa10ebe-25a4-4ad3-8f99-affded343fcd/ierb_a_11205123_f0002_b.jpg)
The two arrows indicate the gap between urethra and puborectalis insertion that can conveniently be palpated to determine muscle integrity.
Reproduced with permission from Citation[61].
![Figure 3. The appearance of the puborectalis muscle in a rendered volume in the axial plane, using translabial 3D ultrasound with speckle reduction imaging.The two arrows indicate the gap between urethra and puborectalis insertion that can conveniently be palpated to determine muscle integrity.Reproduced with permission from Citation[61].](/cms/asset/5efbd0d3-3708-42e5-8e04-37204d21f16c/ierb_a_11205123_f0003_b.jpg)
(A) Shows appearances immediately postpartum, with the avulsed muscle exposed by a large vaginal tear. (B) Shows a rendered volume (axial plane, translabial 3D ultrasound) 3 months postpartum. (C) Shows MRI findings (single slice in the axial plane) at 3.5 months postpartum.
Reproduced with permission from Citation[14].
![Figure 4. Right-sided puborectalis avulsion after normal vaginal delivery at term.(A) Shows appearances immediately postpartum, with the avulsed muscle exposed by a large vaginal tear. (B) Shows a rendered volume (axial plane, translabial 3D ultrasound) 3 months postpartum. (C) Shows MRI findings (single slice in the axial plane) at 3.5 months postpartum.Reproduced with permission from Citation[14].](/cms/asset/8fba29c9-5e10-4de6-b520-bc0ac845499a/ierb_a_11205123_f0004_b.jpg)
(A) Shows a normal muscle, (B) an avulsion injury.
Reproduced with permission from Citation[20].
![Figure 5. Digital palpation of the puborectalis muscle insertion.(A) Shows a normal muscle, (B) an avulsion injury.Reproduced with permission from Citation[20].](/cms/asset/5600a066-f2ed-4df9-bd7d-84fed4047256/ierb_a_11205123_f0005_b.jpg)
L: Left; R: Right.
Reproduced with permission from Citation[20].
![Figure 6. Suggested schematic for the documentation of puborectalis trauma, modified Oxford grading and grading of resting tone.L: Left; R: Right.Reproduced with permission from Citation[20].](/cms/asset/c2221f7b-ef6a-495b-b33c-bfb7997b49ad/ierb_a_11205123_f0006_b.jpg)
It is evident that the pelvic sidewall is smoothly denuded of muscle, that is, that the morphological abnormality documented here is an ‘avulsion’ of the puborectalis muscle insertion.
Reproduced with permission from Citation[61].
![Figure 7. Typical right-sided avulsion injury in a rendered volume, axial plane.It is evident that the pelvic sidewall is smoothly denuded of muscle, that is, that the morphological abnormality documented here is an ‘avulsion’ of the puborectalis muscle insertion.Reproduced with permission from Citation[61].](/cms/asset/7f64f5b9-b5ca-4975-9fef-b0c07c957bca/ierb_a_11205123_f0007_b.jpg)
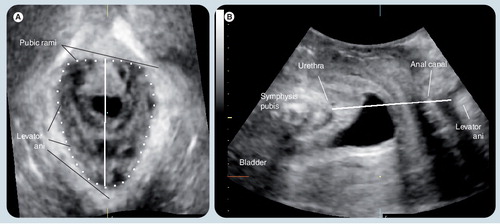
This plane, while not always sufficient to diagnose avulsion injury, defines the levator hiatus, is used to determine hiatal dimensions and distensibility, and serves as a convenient reference plane for tomographic ultrasound imaging.
(A) represents a reference image in the coronal plane. (B–I) Show slices parallel to the plane of minimal hiatal dimensions. (B & C) Are 5 and 2.5 mm below this plane, respectively. (D) Represents the plane of minimal dimensions. (E–I) Are 2.5–12.5 mm above this plane, encompassing the entire insertion of the puborectalis. (B) Is clearly below the muscle insertion (short arrows). (I) Is starting to show much thinner muscle, probably representing iliococcygeus rather than puborectalis (long arrows).
Modified with permission from Citation[37].
![Figure 9. Assessment of the puborectalis muscle by tomographic or multislice ultrasound.(A) represents a reference image in the coronal plane. (B–I) Show slices parallel to the plane of minimal hiatal dimensions. (B & C) Are 5 and 2.5 mm below this plane, respectively. (D) Represents the plane of minimal dimensions. (E–I) Are 2.5–12.5 mm above this plane, encompassing the entire insertion of the puborectalis. (B) Is clearly below the muscle insertion (short arrows). (I) Is starting to show much thinner muscle, probably representing iliococcygeus rather than puborectalis (long arrows).Modified with permission from Citation[37].](/cms/asset/113db7a8-786f-4a41-92f6-213b2f5adc3a/ierb_a_11205123_f0009_b.jpg)
(A) An avulsion on the patient’s right (marked by *). (B) Intact muscle on the patient’s left. (C) Tomographic representation of the puborectalis muscle in the same patient, with the avulsion evident in most slices (marked by *).
Reproduced with permission from Citation[39].
![Figure 10. 2D parasagittal oblique views of the puborectalis muscle obtained by translabial ultrasound.(A) An avulsion on the patient’s right (marked by *). (B) Intact muscle on the patient’s left. (C) Tomographic representation of the puborectalis muscle in the same patient, with the avulsion evident in most slices (marked by *).Reproduced with permission from Citation[39].](/cms/asset/869cf6a0-b9d7-45a2-b3ee-6fb0c1b9c832/ierb_a_11205123_f0010_b.jpg)
FDVD: Vaginal operative forceps or vacuum delivery.
Reproduced with permission from Citation[43].
![Figure 11. Relationship between age at first delivery and levator avulsion.FDVD: Vaginal operative forceps or vacuum delivery.Reproduced with permission from Citation[43].](/cms/asset/71a9873c-3fda-4984-8a9a-ce41bc9cd47a/ierb_a_11205123_f0011_b.jpg)
Antepartum and postpartum ultrasound images (single-slice axial planes in the plane of minimal hiatal dimensions) of a patient with left-sided avulsion after forceps delivery. (A) The hiatal area on maximum Valsalva at 38 weeks was 15.6 cm2. (B) It was measured at 29.3 cm2 at 4 months postpartum.
Reproduced with permission fromCitation[61].
![Figure 12. The effect of levator avulsion on hiatal dimensions.Antepartum and postpartum ultrasound images (single-slice axial planes in the plane of minimal hiatal dimensions) of a patient with left-sided avulsion after forceps delivery. (A) The hiatal area on maximum Valsalva at 38 weeks was 15.6 cm2. (B) It was measured at 29.3 cm2 at 4 months postpartum.Reproduced with permission fromCitation[61].](/cms/asset/e1e34bdd-2893-4c67-a196-2581803c5acd/ierb_a_11205123_f0012_b.jpg)