Figures & data
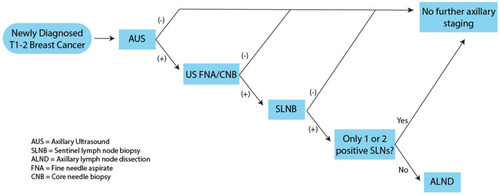
Figure 1 Overview of current algorithms for axillary staging in early stage breast cancer. SLNB is recommended for patients with a clinically negative axilla. If ≥ 3 sentinel nodes are positive, completion ALND is recommended. No further intervention is indicated for ≤ 2 sentinel nodes are positive. US guided FNA/CNB is recommended for patients with a clinically positive axilla. If FNA/CNB is positive, ALND is indicated. If FNA/CNB is negative, SLNB ± ALND is recommended. For patients with a positive FNA/CNB who undergo NAC, SLNB may be considered depending on response to treatment.
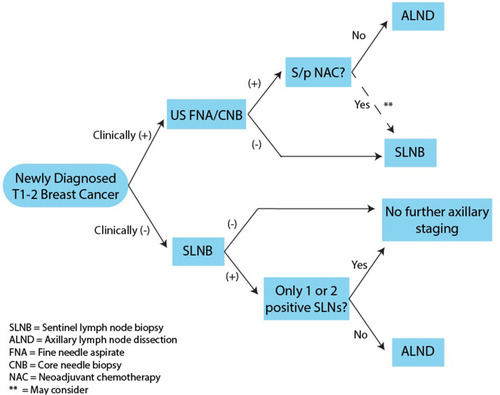
Figure 2 Ultrasound features suggesting metastatic involvement of axillary lymph nodes. Normal lymph nodes have a uniform hypoechoic cortex, central fatty hilum, and smooth margins. Features identified to be predictive of metastatic lymph node disease include increased cortical thickness (OR=3), fatty hilum loss (OR=27), increased diameter, and irregular margins (OR=3). While the features high odds ratios, they are not individually predictive of lymph node metastasis and have poor AUCs.
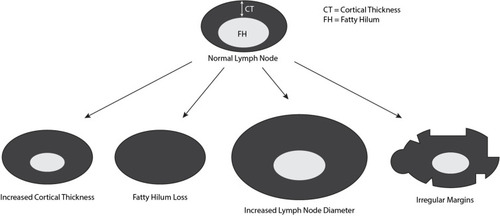
Figure 3 Restaging of the axilla after NAC. ALND has traditionally been recommended for patients with a clinically positive axilla and positive FNA/CNB. For patients who are treated with NAC, evaluation with AUS can help reduce the utilization of ALND and concomitant patient morbidity. Following NAC, AUS can be used to assess response to therapy, If the AUS is negative after NAC, SLNB is recommended with ALND reserved for patients with ≥ 2 positive sentinel lymph nodes.
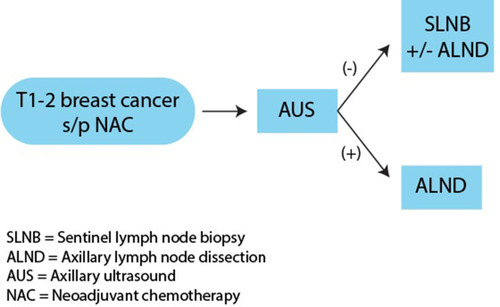
Table 1 Summary of Current Trials Underway Evaluating the Utility of AUS in Breast Cancer Staging
Figure 4 Possible future algorithm for staging of the axilla in early stage breast cancer. Several studies are currently ongoing evaluating the ability of AUS to accurately exclude disease in the axilla. If these studies are successful, the paradigm for axillary staging will evolve. Patients with newly diagnosed T1-2 breast cancer will be evaluated with an AUS. Patients with negative AUS will not require further axillary staging. Patients with a positive AUS will undergo FNA/CNB. Patients with a negative FNA/CNB can be observed. Patients with a positive FNA/CNB should undergo SLNB, possible ALND.