Figures & data
Figure 1 The bone marrow biopsy showed nodular proliferation of neoplastic lymphocytes (A, H&E x 20). Immunohistochemistry revealed the lymphocytes positive for CD23 (B, x 20). Flow cytometry analysis confirmed lymphocytes positive for CD20 and predominantly negative for CD38 (C). FISH study revealed loss ofD13S319 signal, which indicated the deletion of 13q (D).
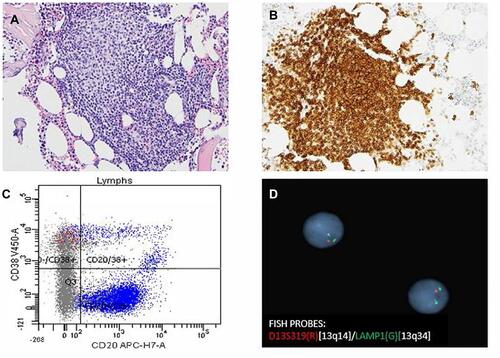
Figure 2 (A) Pretreatment CT imaging showed a left pelvic sidewall mass, pelvic mesenteric lymphadenopathy, and external iliac lymphadenopathy. (B). Pretreatment PET shows hypermetabolic pelvic lesion however unable to accurately measure SUVs in this mass due to concentrated radiotracer within the involved left ureter. (C). Pretreatment CT imaging showed associated left hydronephrosis. (D) Post treatment PET scan after 6 cycles of induction therapy showed low level metabolic activity within the left pelvic sidewall mass, SUV max 2.1, no evidence for recurrence.
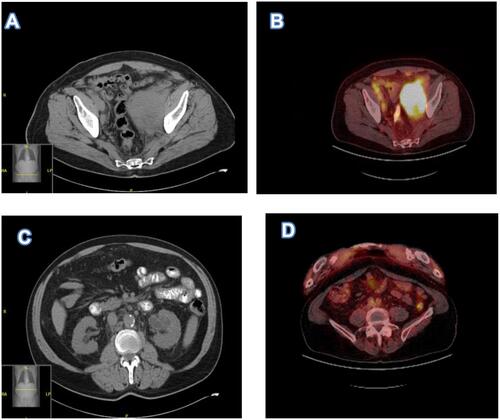
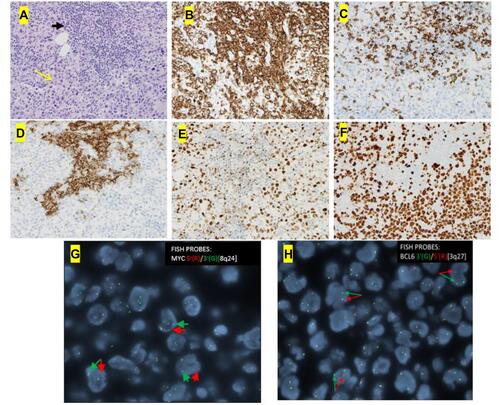
Figure 3 The core needle biopsy of the pelvic mass showed a diffusely infiltrating large atypical cells (yellow arrow) with intermixed clusters of small lymphocytes (black arrow) (A, H&E x 20). Immunohistochemical studies showed both small and large lymphocytes were strongly positive for CD20 (B, x 20). While the small lymphocytes showed aberrant expression of CD5 (C, x 20) and CD23 (D, x 20), the large lymphocytes were negative for CD5 and CD23 but positive for BCL6 (E, x 20) with a high proliferative rate by ki-67 (F x 20). FISH analysis with break-apart probes demonstrated MYC gene rearrangement (G, arrows indicate separation of 5ʹMYC and 3ʹMYC) and BCL6 gene rearrangement (H, arrows indicate separation of 3ʹBCL6 and 5ʹBCL6), which confirmed the diagnosis of “double-hit” large cell lymphoma.