Figures & data
Table 1 Patient Characteristics and Treatment Outcome
Figure 1 (A) Axial non-contrast CT on readmission showing acute right parietal intraparenchymal hemorrhage (short white arrow) with mild surrounding edema. (B) Axial T2-FLAIR MRI obtained the next day shows new abnormalities in the left hemisphere (short white arrows). (C) Associated intraparenchymal hemorrhages (short white arrows) on the axial T2* GRE MRI. (D) Abnormal linear enhancement in the conus medullaris (arrowhead). The hematoxylin and eosin (H&E) stained section of brain biopsy shows focal intravascular infiltrate of neoplastic large lymphocytes ((E) and (F), ×40); and they are positive for CD20 by immunohistochemistry study (IHC) ((G), ×40), which confirms the B cell lineage of the lymphoma.
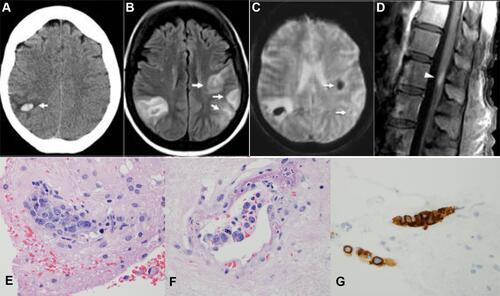
Figure 2 (A) Multiple small subcortical infarcts (short white arrows) on axial DWI MRI at the outside facility. (B) Recurrent small subcortical infarcts (short white arrows) 7 months later on axial DWI MRI. (C) Associated subcortical microhemorrhages (arrowheads) on axial susceptibility-weighted MRI. (D) MR angiography showing focal narrowings in intracranial arteries (arrowheads). The H&E section of spleen demonstrated neoplastic large atypical lymphocytes (black long arrow) filling the sinusoid and small vessels in the red pulp ((E), ×40). Immunostains show the neoplastic lymphocytes positive for CD20 (black long arrow) with a high proliferative rate by Ki-67 (90%) ((F), ×40). The clusters of large lymphocytes within the sinusoid (black long arrow) are highlighted by immunostain of CD20 and ki-67 ((G), ×40).
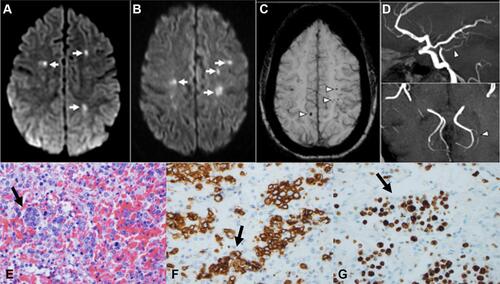
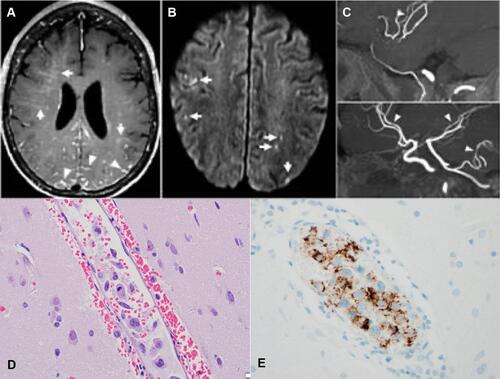
Figure 3 (A) Axial contrast-enhanced T1-weighted MRI showing multifocal subcortical perivascular intraparenchymal enhancement (short white arrows) and leptomeningeal enhancement (arrowheads). (B) Small cortical and subcortical infarcts corresponding to the distribution of perivascular enhancement (short white arrows). (C) MR angiography showing focal narrowing of several intracranial arteries (arrowheads). The H&E section of brain biopsy shows focal intravascular infiltrate of neoplastic large lymphocytes ((D), ×40); and they are positive for CD19 ((E), ×40).