Figures & data
Table 1 Characteristics of tocilizumab and tumor necrosis factor inhibitors
Figure 1 Indirect comparisons of the suppressive effects of tocilizumab and tumor necrosis factor inhibitors on radiographic damage.
Notes: Copyright © 2012. Adapted from Dove Medical Press. Jones G, Darian-Smith E, Kwok M, Winzenberg T. Effect of biologic therapy on radiological progression in rheumatoid arthritis: what does it add to methotrexate? Biologics. 2012;6:155–161.Citation30 In combination with methotrexate (MTX) compared with MTX alone, tocilizumab and all tumor necrosis factor inhibitors are effective at slowing X-ray progression. As monotherapy, adalimumab, etanercept, and tocilizumab are significantly better than MTX, whereas golimumab had no significant effect. The x-axis shows progression of radiographic damage.
Abbreviations: CI, confidence interval; MTX, methotrexate.
Abbreviations: CI, confidence interval; MTX, methotrexate.
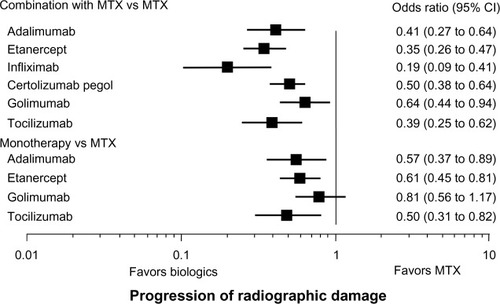
Table 2 Comparative tolerability of tocilizumab with tumor necrosis factor inhibitors
Figure 2 Properties of tocilizumab and tumor necrosis factor inhibitors in the management of rheumatoid arthritis.
Abbreviations: AEs, adverse events; CRP, C-reactive protein; GI, gastrointestinal; MTX, methotrexate; SAA, serum amyloid A; TB, tuberculosis; T-CHO, total cholesterol.
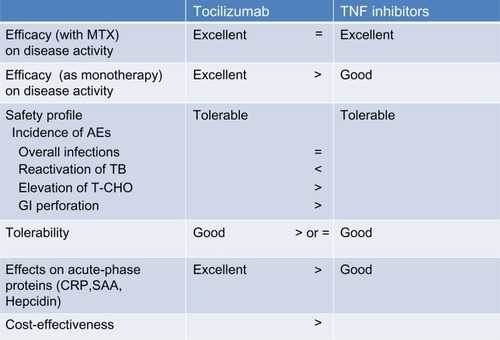
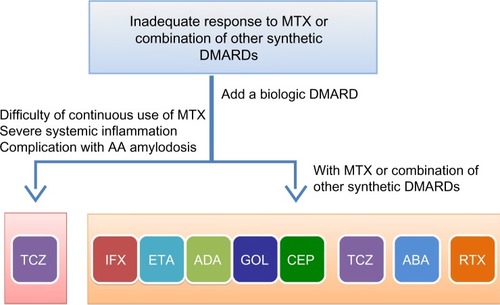
Figure 3 Selection of biologic disease modifying antirheumatic drugs.
Notes: Rheumatoid arthritis patients who fail to respond to methotrexate (MTX) alone or in combination with other synthetic disease modifying antirheumatic drugs (DMARDs) need to be treated with a biologic DMARD. For patients who can continue to receive MTX, any of the seven biologic DMARDs should be selected. These include five tumor necrosis factor inhibitors (infliximab, etanercept, adalimumab, golimumab, and certolizumab pegol), the IL-6 receptor blocker tocilizumab, the T-cell stimulation blocker abatacept, and the B-cell depletory rituximab. Rituximab is recommended to be used for patients who have certain contraindications for other agents such as a recent history of lymphoma, latent tuberculosis with contraindications to the use of chemoprophylaxis, live in a tuberculosis endemic region, or a previous history of demyelinating disease. Tocilizumab may be selected for patients who 1) cannot continue treatment with MTX or other synthetic DMARDs, 2) present with severe inflammatory findings, and 3) have or who are at high risk of developing amyloid A amyloidosis.
Abbreviations: ABA, abatacept; ADA, adalimumab; CEP, certolizumab pegol; DMARDs, disease modifying antirheumatic drugs; ETA, etanercept; GOL, golimumab; IFX, infliximab; MTX, methotrexate; RTX, rituximab; TCZ, tocilizumab.
Abbreviations: ABA, abatacept; ADA, adalimumab; CEP, certolizumab pegol; DMARDs, disease modifying antirheumatic drugs; ETA, etanercept; GOL, golimumab; IFX, infliximab; MTX, methotrexate; RTX, rituximab; TCZ, tocilizumab.