
Figures & data
Figure 1 Lentigo maligna(LM)/LM melanoma (LMM) clinical presentations. (A) LM presenting as a large irregularly pigmented patch in the forehead with central regression and ill-defined borders. (B) LM arising on the right cheek clinically simulating a seborrheic keratosis. (C) Large LM occurring on the nose and surrounded by chronically sun damaged skin. (D) Light brown patch with ill-defined borders in a fair-skinned individual corresponding to a LMM that can clinically be easily mistaken for solar lentigo. (E) Extrafacial LMM affecting the upper back presenting as an isolated large homogeneous brown patch with irregular borders. (F) Nodular melanoma arising on a previous LM (note the brown pigment surrounding the nodule corresponding to the in situ component).
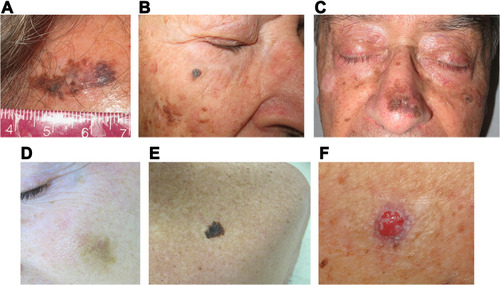
Table 1 Lentigo Maligna (LM)/LM Melanoma (LMM) Differential Diagnosis: Clinical Presentation and Dermoscopy
Figure 2 Lentigo maligna(LM)/LM melanoma (LMM) dermoscopic findings. (A) Facial LM with an annular-granular pattern consisting of brown dots scattered around adnexal openings. (B) LM showing a large blotch with the blue-black sign. (C) LM on the scalp with follicle obliteration and central regression (gray peppering or granularity). (D) Facial LM with an annular-granular pattern around adnexal openings and follicle obliteration. (E) Brown lines coalescing to form rhomboids (angulated lines) around adnexal ostial openings at the periphery of this LM. Also, an asymmetric distribution of pigment surrounding the follicular openings can be seen. (F) Extrafacial LM with presence of network and atypical dots. Note the absence of adnexal openings in extrafacial skin.
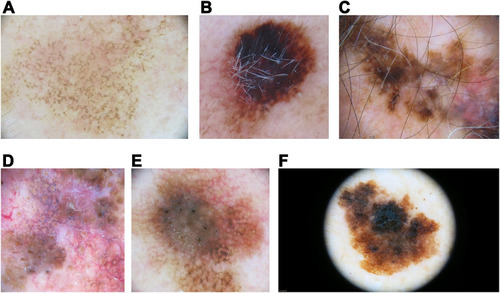
Figure 3 Schiffner progression model fo LM/LMM. Initially asymmetric pigmentation and dots around the follicle are seen (A), which later evolve to rhomboidal structures (B) and finally form homogeneous pigmented areas and cause obliteration of the follicular openings (C). Adapted with permission from Dermoscopedia (https://creativecommons.org/licenses/by-nc-sa/4.0/).Citation158

Figure 4 Reflectance confocal microscopy images of a lentigo maligna. The epidermis (depth ~50 µm) shows numerous pleomorphic pagetoid cells composed of large round cells (arrowheads, A) as well as dendritic cells (star, A), which can invade the hair follicles (star, B). At the dermal-epidermal junction (depth ~150 µm), one can also identify disarrangement of the basal layer as well as large plump cells which correlate with melanophages (arrowhead, B), and junctional thickenings than can radiate from the hair follicles adopting a medusa head-like () structure (arrowhead, C), or a mitochondria-like structure (asterisk, D). (white scale bars: 250 µm).
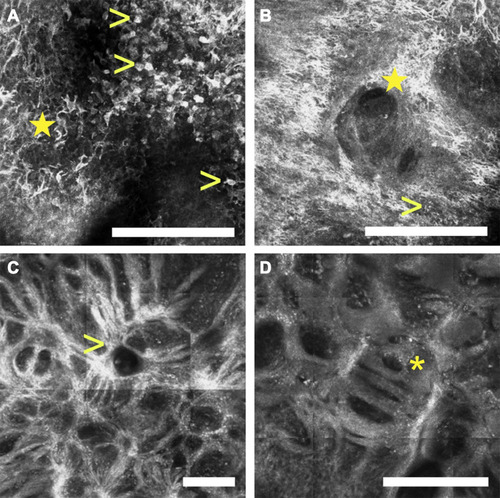
Table 2 In vivo Confocal Features for LM Diagnosis
Figure 5 (A) Histological pictures of lentigo maligna. Lentigo maligna in the radial growth phase. Solar elastosis (arrow), a patchy lymphocytic infiltrate and melanophages are seen in the dermis (+ sign). An atrophic epidermis (asterisk) and an increased density of melanocytes along the dermal-epidermal junction can be seen, some of them with variable nuclear atypia (arrowheads). Hematoxylin-eosin stain10x. (B) Extrafacial lentigo maligna on chronically sun-damaged skin. Atrophic epidermis (asterisk), prominent solar elastosis (arrow) and increased density of junctional pleomorphic melanocytes forming asymmetric nests with pagetoid growth of single melanocytes (arrowheads). Dermal inflammatory infiltrate with melanophages (+ sign). Hematoxylin-eosin stain10x.
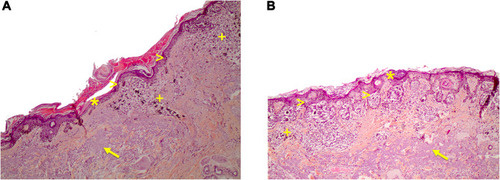
Table 3 Evidence-Based Recommendations for Lentigo Maligna (LM)