Figures & data
Figure 1 High-frequency HIFU applied to the human skin.Citation13 At 20 MHz, the focal zone is sufficiently small to prevent damages to the deeper part of the dermis and subcutaneous layer below.
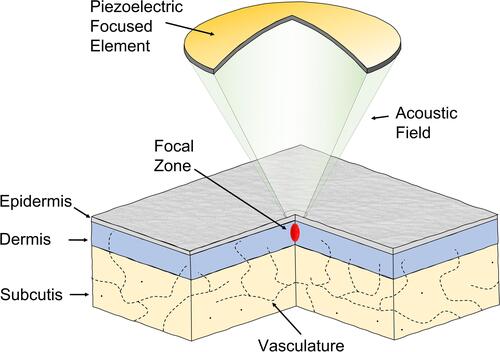
Figure 2 Dynamics in removal of seborrheic keratosis by high-frequency HIFU. (A) An epidermal seborrheic keratosis (SK) is located in the skin. (B) Shoulder-by-shoulder HIFU doses are placed to cover the SK-field including a small margin. (C) A necrotic volume containing SK cells is formed directly after treatment. (D) The wound crust is spontaneously released after 1–2 weeks after damaged cells have been replaced.
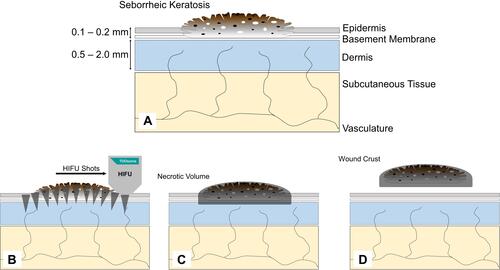
Figure 3 TOOsonix HIFU system operating at 20 MHz. The handpieces have an integrated real-time video camera allowing accurate control and monitoring of the treatment.

Figure 4 (A) Overview of anatomical location of lesions selected for HIFU treatment. (B) Anatomical location for each subject in the study.
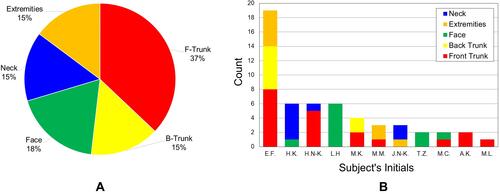
Figure 5 Typical dermoscope appearance of seborrheic keratosis. (A) Before HIFU treatment. (B) Directly after treatment. Whitening of the epidermis and denaturation of the superficial skin structure as a reaction to the thermal and mechanical effects of HIFU can be observed.
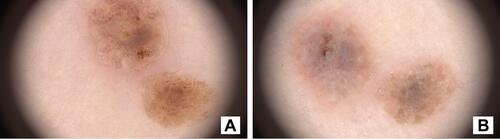
Table 1 Overview of Subjects and Results of HIFU Treatments (Full Data are Available as Additional Information from the Journal Internet Page)
Figure 6 Summary chart of dermoscopic features detected at follow-up.
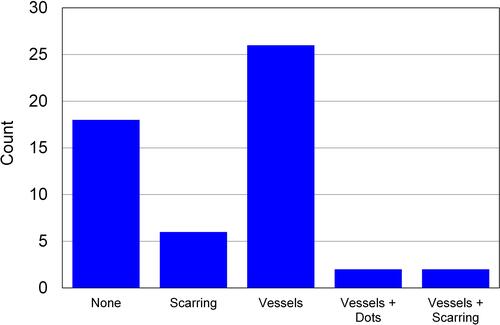
Figure 7 Case 1. (A and B) Macro-photo and dermoscope pictures of a large and thick seborrheic keratosis before HIFU. (C and D) Macro-photo and dermoscope pictures 6 weeks after initial HIFU treatment. The seborrheic keratosis has clearly reduced in thickness and the majority of brown clods and coiled vessels have been removed. The lesion is however still clearly visible, in particular in the periphery of the original lesion. A second repeat treatment was administered. (E and F) Macro-photo and dermoscope picture at follow-up visit 10 weeks after first treatment (4 weeks after second treatment). The visual appearance is significantly improved, but seborrheic keratosis is still visible, and a third treatment will be needed to fully remove the lesion.
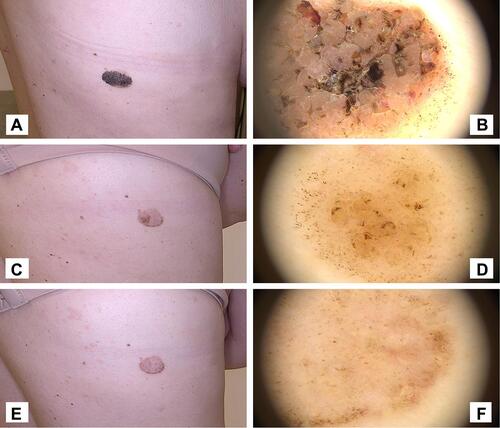
Figure 8 Case 2. (A and B) Macro-photo and dermoscope picture of large seborrheic keratosis on left breast before HIFU. (C and D) Macro-photo and dermoscope picture of treated area at control visit 4 weeks after HIFU treatment.
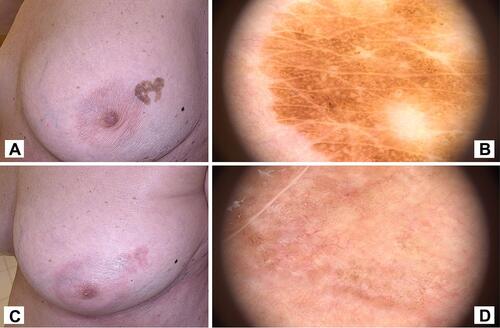
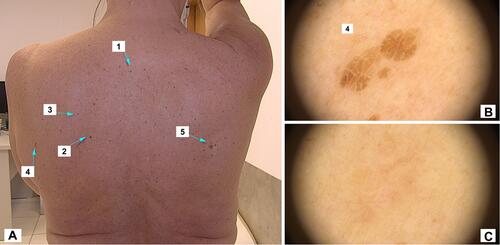
Figure 9 Case 3. (A) Macro-photo of 5 selected seborrheic keratoses lesions for HIFU treatment. (B) Dermoscope picture of lesion number 4 before HIFU. (C) Dermoscope picture of lesion number 4 at the control visit 5 weeks after treatment.